- Incidence of Ewing's sarcoma
- Risk factors for developing Ewing's sarcoma
- Diagnosis of Ewing's sarcoma
- Determination of the stage (prevalence) of Ewing's sarcoma
- Treatment of Ewing's sarcoma
- After completion of treatment
Ewing's sarcoma ranks second in frequency among malignant bone tumors in children (after osteogenic sarcoma) and was first described by D. Ewing in 1921 and named after the author.
This tumor is rare in children under 5 years of age and in adults over 30 years of age. Most often, this tumor occurs in adolescents aged 10 to 15 years. There are cases of extraosseous Ewing's sarcoma with soft tissue involvement.
Another childhood tumor, primitive neuroectodermal tumor (PNET), shares many features with osseous and extraosseous Ewing sarcoma, which can primarily affect both bone and soft tissue. All of these tumors develop from the same type of cells.
Bone Ewing sarcoma accounts for 87%, extraosseous Ewing sarcoma 8% and PNET -5%.
Typically, such tumors develop in the central part of the long bones of the upper and lower extremities, but can also be detected in the pelvic bones and in the bones and soft tissues that form the chest.
Incidence of Ewing's sarcoma
Among malignant tumors in children, Ewing's sarcoma accounts for 1.8% and is the second most common among malignant bone tumors in children (10-15%).
Every year in the United States, this tumor is diagnosed in 150 children and adolescents. Males are more often affected by the disease.
There is some connection between the occurrence of Ewing's sarcoma and the presence of abnormalities of the skeleton and genitourinary system.
In 30% of cases, at the time of diagnosis there is already metastatic damage to the lungs and bones.
Description of palliative “chemistry”
The fundamental principle of this therapy is not the complete elimination of pathology, but only a reduction in tumor size. Thus, it is possible to reduce the severity of complications and prolong the life of a cancer patient. Palliative chemotherapy treatments are prescribed for people who suffer from incurable types of sarcomas. The treatment process inhibits the progression of cancer pathology and helps to increase life expectancy. The period of increase may vary: from 3-4 months to several years. Much depends on the therapy used, which may also be experimental (see the corresponding section).
Risk factors for developing Ewing's sarcoma
Currently, several risk factors are known to be associated with the occurrence of Ewing's sarcoma.
Floor. Ewing's sarcoma is slightly more common among boys than girls.
Age. In 64% of cases, Ewing's sarcoma occurs between the ages of 10 and 20 years.
Race. Ewing's sarcoma is most often observed in the white population.
Prevention of Ewing's sarcoma, like most other childhood tumors, is currently impossible, since the lifestyle of children and their parents does not affect the incidence of this tumor.
Prevention of bone cancer
There are no specific methods for preventing bone neoplasm. As general measures we can recommend:
- Quit smoking and abusing alcoholic beverages.
- Lead a physically active lifestyle.
- Maintain immunity: taking herbal preparations that stimulate the immune system, hardening water procedures, regularly taking vitamin-mineral complex tablets.
- Stick to a balanced diet.
- Regularly undergo preventive medical examinations.
However, it should be borne in mind that a healthy lifestyle does not guarantee a reduction in the risk of developing any types of malignant diseases. Therefore, if you suspect bone cancer, even mild symptoms should alert you. Seeking specialized professional medical help allows you to start therapy early and increase the effectiveness of treatment measures.
Diagnosis of Ewing's sarcoma
Signs and symptoms of Ewing's sarcoma
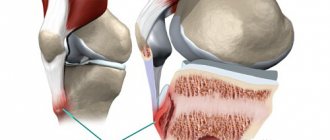
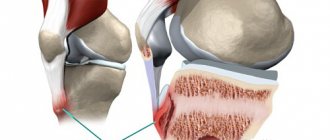
The most common symptom of Ewing's sarcoma is pain, which occurs in 85% of children with bone lesions. Pain can be caused either by the spread of the process to the periosteum or by a fracture of the affected bone.
60% of patients with Ewing's sarcoma of bone and almost all patients with extraosseous tumors develop a swelling or induration. In 30% of cases, the tumor is soft and warm to the touch. Patients have elevated body temperature.
These signs and symptoms can also be observed with bruises and inflammation of bone tissue, but they disappear after treatment with antibiotics.
With advanced (metastatic) Ewing's sarcoma, patients may complain of increased fatigue and weight loss. In rare cases, for example, when the spine is damaged, severe weakness in the lower extremities and even paralysis are possible.
Peripheral blood analysis. The detection of tumor cells in the patient's blood indicates bone marrow damage in Ewing's sarcoma.
Blood chemistry. An increase in the level of LDH (lactate dehydrogenase) gives the right to suspect a metastatic process in a patient with Ewing's sarcoma.
X-ray examination of bones makes it possible to diagnose Ewing's sarcoma with some certainty.
X-ray examination of the chest makes it possible to detect metastases of Ewing's sarcoma in the lungs.
Computed tomography (CT) (sometimes with additional contrast) of the bones of the chest and abdominal cavity makes it possible to clarify the location and size of the tumor and identify the presence of metastases in the lungs, lymph nodes and liver.
Magnetic resonance imaging (MRI) provides additional information about the bone marrow, muscle and connective tissue around the affected bones and helps determine the extent of the tumor.
Radionuclide scanning (scintigraphy) using technetium-99 reveals damage to other bones and soft tissues.
Bone marrow puncture and biopsy are necessary to identify its involvement in Ewing's sarcoma.
Tumor biopsy (taking a piece of tumor for examination) is the final and mandatory method for clarifying the diagnosis of Ewing's sarcoma
Elimination of pathology and possible prognosis
One hundred percent relief from this disease is possible only if the cancer focus is removed. This is possible when the tumor is small and there is no damage to vital organs. In addition, single metastases within the lung, bone and liver tissues can be completely cured. In fact, the most positive outcome is possible only in the early stages of the oncological process.
When cancer is advanced, even after taking therapeutic measures, survival rates are only 20% (and this is the maximum). Frequent recurrent manifestations are likely.
Determination of the stage (prevalence) of Ewing's sarcoma
Clarifying the stage of Ewing's sarcoma is important both for determining the prognosis (outcome) of the disease and for planning treatment. Ewing's sarcoma has two stages of disease: localized and metastatic.
In the localized stage, the tumor is limited to the tissue from which it originated, but may also spread to surrounding muscles and tendons.
The absence of visible metastases does not exclude the presence of small foci (micrometastases) of the tumor, which can only be detected by microscopic examination.
The metastatic stage means the tumor has spread to the lungs, bones, bone marrow, lymph nodes, and liver.
Symptoms
First of all, the patient is tormented by aching, increasing pain. Holding a limb in one position does not relieve pain. There is swelling of the affected area. This swelling quickly covers the entire affected limb; joints may be involved in the pathological process. Often the affected area has higher temperatures.
Impairment of motor function in an arm or leg may be present (depending on location). Also, there are general signs: weakness, weight loss. Sometimes the patient suffers from uncontrollable urination. Paralysis of the arms and legs is possible (if the cancer focus is on the spine).
In addition, the size of the lymph nodes may increase. Nerve fibers may lose their original sensitivity. Also, hemoptysis, difficulty breathing, and atypical gait may occur.
Treatment of Ewing's sarcoma
OPERATION
The type of surgery chosen depends on the location of the tumor and the effect of the surgery on the function of the affected body part.
In many cases, the affected bone or soft tissue can be completely removed surgically without affecting organ function. In other cases, preservation of organ function after complete removal of tumor tissue is impossible.
If many years ago, Ewing's sarcoma of the upper and lower extremities was treated with amputation, now preservation operations are most often performed. In this case, the removed bones and joints are replaced with grafts or prostheses. Safe operations are performed even on patients with damage to the pelvic bones.
In patients with Ewing's sarcoma with damage to vital nerves and blood vessels, radiation therapy may be used instead of surgery.
If Ewing's sarcoma is localized in the chest, the tumor is removed along with several ribs, which are replaced with synthetic material.
Metastatic nodes in the lungs are removed during a thoracotomy operation. After surgery, such patients undergo radiation therapy to the lung tissue.
Among the immediate and long-term consequences of surgical treatment of Ewing's sarcoma, poor wound healing and infectious complications should be noted. This is due to previous chemotherapy and radiation. After surgery, many patients with Ewing's sarcoma require restorative treatment.
Chemotherapy for patients with Ewing's sarcoma is carried out using antitumor drugs, usually administered intravenously and rarely orally. This treatment method is used for all patients, regardless of the stage of the disease.
This is explained by the fact that even patients with a localized process may have micrometastases that can only be detected by microscopic examination. Therefore, avoiding chemotherapy in patients with localized stage will eventually lead to the growth of these micrometastases.
For chemotherapy of Ewing's sarcoma, various combinations (combinations) of anticancer drugs are used, which are prescribed every 3-4 weeks.
First, a combination of drugs such as vincristine, adriamycin (doxorubicin) and cyclophosphamide is used. After the side effects of chemotherapy subside, a second combination is given, including ifosfamide and etoposide. Such chemotherapy cycles are repeated 4-5 times.
Chemotherapy can be accompanied by various side effects such as nausea, vomiting, loss of appetite, baldness, damage to the oral mucosa and bladder, increased susceptibility to infection, menstrual irregularities, infertility, and damage to the heart muscle.
The most serious, although rare, complication of chemotherapy may be the development of a second malignancy, in particular acute myeloid leukemia.
RADIATION THERAPY
In patients with Ewing's sarcoma, external irradiation with high-energy sources is used. This tumor is highly sensitive to radiation, and most patients can be cured with a combination of chemotherapy and radiation.
The total dose of radiation therapy to the lesion is usually 45-55 gray. If indicated, the lungs are irradiated, but the doses of radiation therapy are reduced.
A serious complication of radiation therapy is impaired bone growth. Moreover, the younger the child, the more pronounced the side effects and complications. Radiation therapy can cause limb shortening, facial deformation, etc.
Irradiation of the pelvic area may damage the bladder and colon. Radiation therapy to the joint area can limit its function due to scarring.
Side effects and complications of radiation therapy when affecting the spinal cord and brain appear after 1-2 years and consist of headaches and deterioration of mental activity.
High doses of radiation therapy (over 60 gray) in 20% of cases lead to the development of a second malignant tumor.
Bone marrow and peripheral stem cell transplantation
Recently, patients with a poor prognosis, in particular those with metastases to the bones and bone marrow, with a survival rate of less than 10%, have been treated with more intensive treatment - high-dose chemotherapy with body irradiation and bone marrow or peripheral stem cell transplantation. This approach makes it possible to cure more than 30% of patients with a metastatic process.
Palliative surgery methods
The staff of the Interventional Oncology Department perform palliative surgical interventions.
1. Venous and arterial port systems are implanted, which are designed to administer chemical agents. These systems are recommended for cancer patients who will have to receive chemotherapy drugs for a very long time. The main advantages of this approach are: the availability of quick and trouble-free access to the veins (this is especially important when obtaining blood mass or administering medications), reducing the likelihood of phlebitis, ensuring repeated administration of chemotherapy drugs, providing psychological comfort for people who are terrified of needles, the possibility of long-term use system, complete absence of any discomfort.
2. Nephrostoma is applied, thanks to which urine is drained from the kidneys. Often the procedure is done through open surgery. However, the most popular to this day is percutaneous puncture nephrostomy, which uses X-ray or ultrasound control.
3. They perform procedures related to drainage or stenting of bile ducts.
4. Vava filters are installed to prevent thromboembolism of the pulmonary artery.
Bibliography:
- Juergens C, Weston C, Lewis I, Whelan J, Paulussen M, Oberlin O, Michon J, Zoubek A, Jürgens H, Craft A: Safety assessment of intensive induction with vincristine, ifosfamide, doxorubicin, and etoposide (VIDE) in the treatment of Ewing tumors in the EURO-EWING 99 clinical trial. Pediatric blood & cancer 2006, 47: 22 [PMID: 16572419] JüR2006
- Kaatsch P, Spix C: German Childhood Cancer Registry - Jahresbericht / Annual Report 2015 (1980-2014). Institut für Medizinische Biometrie, Epidemiologie und Informatik (IMBEI), Universitätsmedizin der Johannes Gutenberg-Universität Mainz 2015 [URI: www.kinderkrebsregister.de] KAA2015a
- Dirksen U, Jürgens H: Ewing-Sarkome des Kindes- und Jugendalters. S1-Leitlinie der Gesellschaft für Pädiatrische Onkologie und Hämatologie (GPOH) AWMF online 2014 [URI: www.awmf.org] DIR2014
- Haeusler J, Ranft A, Boelling T, Gosheger G, Braun-Munzinger G, Vieth V, Burdach S, van den Berg H, Jürgens H, Dirksen U: The value of local treatment in patients with primary, disseminated, multifocal Ewing sarcoma ( PDMES). Cancer 2010, 116: 443 [PMID: 19924786] HAE2010
- Burkhardt B, Reiter A, Landmann E, Lang P, Lassay L, Dickerhoff R, Lakomek M, Henze G, von Stackelberg A: Poor outcome for children and adolescents with progressive disease or relapse of lymphoblastic lymphoma: a report from the Berlin-Frankfurt -muenster group. Journal of clinical oncology 2009, 27: 3363 [PMID: 19433688] BUR2009
- Wagner LM, McAllister N, Goldsby RE, Rausen AR, McNall-Knapp RY, McCarville MB, Albritton K: Temozolomide and intravenous irinotecan for the treatment of advanced Ewing sarcoma. Pediatric blood & cancer 2007, 48: 132 [PMID: 16317751] WAG2007
- Gerth HU, Juergens KU, Dirksen U, Gerss J, Schober O, Franzius C: Significant benefit of multimodal imaging: PET/CT compared with PET alone in staging and follow-up of patients with Ewing tumors. Journal of nuclear medicine : official publication, Society of Nuclear Medicine 2007, 48: 1932 [PMID: 18006618] GER2007
- Germeshausen M, Skokowa J, Ballmaier M, Zeidler C, Welte K: G-CSF receptor mutations in patients with congenital neutropenia. Current opinion in hematology 2008, 15: 332 [PMID: 18536571] GER2007
- Bernstein M, Kovar H, Paulussen M, Randall RL, Schuck A, Teot LA, Jürgens H: Ewing's sarcoma family of tumors: current management. The oncologist 2006, 11: 503 [PMID: 16720851] BER2006
- Hunold A, Weddeling N, Paulussen M, Ranft A, Liebscher C, Jürgens H: Topotecan and cyclophosphamide in patients with refractory or relapsed Ewing tumors. Pediatric blood & cancer 2006, 47: 795 [PMID: 16411206] HUN2006
- Hawkins DS, Schuetze SM, Butrynski JE, Rajendran JG, Vernon CB, Conrad EU 3rd, Eary JF: [18F]Fluorodeoxyglucose positron emission tomography predicts outcome for Ewing sarcoma family of tumors. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2005, 23: 8828 [PMID: 16314643] HAW2005
- Dirksen U, Poremba C, Schuck A: Knochentumoren des Kindes-und Jugendalters. Der Onkologe 2005, 10: 1034 DIR2005
- Niemeyer C, Kontny U: Tumoren der Ewing-Sarkom-Familie, in: Gutjahr P (Hrsg.): Krebs bei Kindern und Jugendlichen. Deutscher Ärzte-Verlag Köln 5. Aufl. 2004, 491 [ISBN: 3769104285] NIE2004
- Schuck A, Ahrens S, Paulussen M, Kuhlen M, Konemann S, Rube C, Winkelmann W, Kotz R, Dunst J, Willich N, Jürgens H: Local therapy in localized Ewing tumors: results of 1058 patients treated in the CESS 81, CESS 86, and EICESS 92 trials. Int J Radiat Oncol Biol Phys 2003, 55: 168 [PMID: 12504050] SCH2003g
- Paulussen M, Frohlich B, Jürgens H: Ewing tumor: Incidence, prognosis and treatment options. Paediatr Drugs 2001, 3: 899 [PMID: 11772151] PAU2001c
Ewing's sarcoma: brief information (336KB) author: Dipl.-Biol. Maria Yiallouros, PD Dr. med. Gesche Tallen Stand: 07/14/2016