Our experience in treating impression fractures of the tibial condyles
The results of treatment of impression-compression fractures of the tibial condyles using a clinically proven method and device for repositioning the articular surface developed by the authors are presented. Excellent and good results were obtained in 88.6% of cases, which is 1.2 times higher than previously presented data in the specialized literature.
Our experience of treating impressional fractures condyles of the tibia
Results of treatment of impression-compressional fractures of condyles of the tibia with application by the developed authors, clinically reasonable method and apparatus for repositioning of the articular surface are presented. Excellent and good results were obtained in 88.6% of cases, which is 1.2 times higher than previously reported data in the special literature.
Fractures of the knee joint area are severe fractures of the bones of the limb. The frequency of such fractures, according to various authors, ranges from 4 to 6.1% of all fractures of the lower extremities [1, 2, 4]. Features of fractures of this location include the location of the fracture plane inside the joint, often accompanied by damage to soft tissue elements. Violation of the congruence of the articular surfaces that make up the knee joint aggravates the nature of the damage and the course of the recovery process. The healing of fractures in the knee joint area often occurs with the formation of excess regenerate tissue, which leads to deformation of the joint and disruption of the congruence of the articular surfaces, and is the cause of the development of stiffness and deforming arthrosis of the joint. The presence of intra-articular hematomas contributes to the formation of adhesions and scars, which can cause persistent contractures of the knee joint. The complexity of fractures in the knee joint area determines the difficulty of repositioning and ensuring adequate stable fixation of fragments during the healing period.
Most authors indicate a significantly higher incidence of tibial condyle fractures compared to femoral condyle fractures. According to O.V. Oganesyan (2005, 2008), fractures of the proximal articular end (condyles) of the tibia account for up to 7.0% of all skeletal bone fractures. The condyles of the tibia are less resistant to force than the condyles of the femur, which is explained by the anatomical features of the metaepiphysis of the femur and tibia [2, 8, 9].
A characteristic feature of most fractures of the tibial condyles is the formation at the time of injury of a primary defect in the cancellous bone of the condyles, otherwise, the zone of primary indentation of the articular surface of the bone plateau, which in most classifications is defined as impression-compression fractures [8, 9].
Treatment of fractures of the knee joint area is a difficult task. Various complications and unsatisfactory treatment outcomes, according to various authors, account for about 50.0% [5, 7, 8]. The surgical method is the main one in the treatment of impression-compression fractures of the knee joint [2, 4, 7, 10].
Since the mid-60s - early 70s of the last century, the method of transosseous osteosynthesis using external fixation devices and, first of all, the method of G.A. has been successfully developing in our country. Ilizarov, which has become the most optimal, including for the treatment of fractures of the knee joint [2, 3, 5, 6, 10]. The advantages of the transosseous osteosynthesis method are as follows: firstly, the Ilizarov apparatus allows you to achieve precise reposition with the elimination of all types of displacements and with minimal tissue trauma without compromising blood circulation in the damaged limb segment; secondly, it provides controlled osteosynthesis with the ability to correct the position of fragments during the treatment process. Stable fixation of fragments in the apparatus does not exclude, in many cases, the loading of the injured limb and the possibility of early movements in the joints, which is the prevention of the development of contractures of the joints of the lower extremities. Methods developed at the Russian Research Center "WTO" named after Academician G.A. Ilizarov, made it possible to further improve the method of transosseous osteosynthesis.
At the same time, the developed classical methods of osteosynthesis with the Ilizarov apparatus are not without certain disadvantages, primarily the inability to use it in the treatment of impression-compression fractures of the tibial condyles, which is associated with its constructive abilities. Within the walls of the Research Center “VTO”, the PCOS method was further developed. Original configurations of rod and pin-and-rod external fixation devices based on the Ilizarov apparatus have been developed and are successfully used in clinical practice, which have improved the outcomes of treatment of fractures of the knee joint, including impression-compression ones.
However, the problem of treating fractures of the knee joint cannot be considered completely resolved. In this regard, we have made an attempt to improve the results of treatment of fractures of the knee joint by improving treatment methods and creating clinically proven methods and devices.
In the department of emergency traumatology of the National Research Center for Clinical Hospital "VIO", 45 patients with impression-compression fractures of the tibial condyles aged from 20 to 70 years were treated. The structure of fractures according to the mechanism of injury is represented by simple fractures of the internal and external condyles due to depression - 17 (38%) and 20 (44%). In 8 cases (18%) fractures of both condyles were observed. For the treatment of this group of patients, the method of transosseous osteosynthesis was chosen using a device we developed that ensures congruence and restoration of the articular surfaces of the bones of the knee joint (RF patent for utility model No. 98896).
This task was achieved due to the fact that in the device for repositioning the articular surface, containing a hollow cylindrical body with a cutting edge and a pusher placed inside it with the possibility of longitudinal movement, the diameter of the pusher corresponds to the inner diameter of the body. The pusher is equipped with a locking head, while the body is equipped with a removable support in the form of a cylindrical rod, at one end of which there is an annular groove with a split ring placed in it, and at the other - a cylindrical head with a handle installed perpendicularly in it (Fig. 1).
Figure 1. Device for repositioning the articular surface: a) diagram; b) appearance of the device (RF utility model patent No. 98896)
A)
b)
The device was used as follows (Fig. 2 a, b, c): after preparing the surgical field, surgical access is carried out: an incision is made along the anterior outer surface of the damaged tibial condyle, exposing the proximal epimetaphysis of the tibia with a rasp.
Figure 2 (a, b, c). Method and device for repositioning the articular surface (Utility model patent No. 98896)
A)
b)
V)
In the paracapsular zone, the anterior section of the meniscus is cut off, which is sutured after osteosynthesis. A removable support is installed in the device body. A visual inspection of the fracture is performed.
On the extra-articular side of the condyle, the device is installed in the direction of the conditional center of indentation. Holding the device by the handle, strike the fixing head of the support with a hammer, moving the device to the desired level . After the body is deepened into the condyle to the required depth, the support is removed from the cylindrical hollow body and replaced with a pusher. The pusher is advanced along the cylindrical hollow body, manually or using a hammer, thereby pushing the bone cylinder located inside the body to the level of the articular surface of the condyle.
Reposition control is carried out visually. The device is removed from the operational area. The defect of the bone substance of the condyle from below is filled with an autograft or osteoinductive material and fixed with knitting needles in the support of the external fixation apparatus. The wound is sutured according to general surgical rules and drained.
Analysis of the treatment outcomes of patients with impression-compression fractures of the tibial condyles indicates the relative majority of excellent and good treatment outcomes when using the transosseous osteosynthesis method with external fixation devices developed by us - 88.6% of the total number, which is 1.2 times higher, according to published earlier than the number of positive outcomes when using classic Ilizarov apparatus configurations.
Let's give a clinical example
Patient G., born in 1973, was treated in the traumatology department No. 1 of the State Autonomous Institution of the Republican Clinical Hospital of the Ministry of Health of the Republic of Tatarstan from 10/19/11 to 11/23/11. Being the driver of a car, I got into an accident. Delivered to the emergency department by ambulance. Diagnosis: closed impression-compression fracture of the lateral condyle of the left tibia. On October 26, 2011, an operation was performed - open transosseous osteosynthesis using an external fixation device for an impression-compression fracture of the lateral condyle of the left tibia. Reposition of the condyle was performed using a device developed by us (Fig. 3 a-d). After achieving reposition, an external fixation device was installed.
Figure 3. Patient G., born in 1973. Diagnosis: closed impression-compression fracture of the lateral condyle of the left tibia: a) radiograph before surgery: b, c - stage of the operation, d - during treatment
A)
b)
V)
G)
Thus, the use of the method and device we developed for the treatment of impression-compression fractures of the knee joint area made it possible to achieve both precise reposition with the elimination of all types of displacements and restoration of the anatomy of the damaged limb segment, and in the vast majority of cases, stable fixation of the proximal articular end of the tibia on period of fusion. The technology we have developed allows us to restore the congruence of the articular surfaces of the knee joint, which in turn sharply reduces the development of gonarthrosis and disability.
H.Z. Gafarov, A.L. Emelin
Kazan State Medical Academy
Gafarov Khaidar Zainullovich - Doctor of Medical Sciences, Professor, Head of the Department of Traumatology and Orthopedics
Literature:
1. Balakina V.S. Intra-articular fractures of the bones of the knee joint / V.S. Balakina; LITO named after. R.R. Vredena: V.G. Weinstein (ed.) and others // Intra-articular fractures: - L. Medgiz, 1958. - P. 138-179.
2. Gorodnichenko A.I. Treatment of peri- and intra-articular fractures of the knee joint with devices / A.I. Gorodnichenko // New technologies in medicine. - Kurgan, 2000. - Part 1. - P. 62-63.
3. Kaplunov O.A. Transosseous osteosynthesis according to Ilizarov in traumatology and orthopedics / O.A. Kaplunov. - M.: GEOTAR-Media, 2002. - P. 62-78.
4. Linnik S.A. Indications and methods of treatment of patients with fractures of the condyles of the knee joint / S.A. Linnik, A.M. Khlynov, K.A. Novoselov and others // Bulletin of the All-Union Guild of Prosthetists and Orthopedists. - Special release. St. Petersburg, 2009. - P. 34.
5. Nigmatullin N.K. Transosseous osteosynthesis in the treatment of fractures in the knee joint / K.K. Nigmatullin // Genius of Orthopedics, 1996. - No. 1. - P. 71-73.
6. Noskov V.K. Treatment of patients with fractures of the condyles of the knee joint bones using the Ilizarov apparatus / V.K. Noskov // Orthopedist, traumatol., 1988. - No. 9. - P. 26-28.
7. Oganesyan O.V. Treatment of chronic fractures of the tibial condyles using a hinge-distraction device / O.V. Oganesyan // Bulletin of traumatology. and orthopedist. them. N.N. Priorova, 2005. - No. 2. - P. 53-56.
8. Plotkin G.L. The problem of impression fractures of the tibial condyles / G.L. Plotkin, V.P. Moskalev, A.A. Domashenko et al. // Bulletin of the All-Union Guild of Prosthetists and Orthopedists. - Special release. St. Petersburg, 2009. - P. 52.
9. Khlynov A.M. Causes of intra-articular fractures of the condyles of the knee joint / A.M. Khlynov, E.G. Lapshinov, F.V. Artemyev et al. // Bulletin of the All-Union Guild of Prosthetists and Orthopedists. - Special release. St. Petersburg, 2009. - P. 69.
10. Shelukhin N.I. Treatment of intra-articular fractures of the condyles of the femur and tibia using various methods / N.I. Shelukhin // Outpatient surgery: Russian quarterly scientific and practical publication. magazine. - St. Petersburg: JSC Rosmedium - North-West, 2004. - No. 1/2. — P. 37-38.
Symptoms
These fractures are easily identified. Specialists initially carefully study the characteristic symptoms of damage:
- Presence of hemarthrosis;
- Soreness;
- Leg deformity;
- Improper functioning of the joint;
- Lateral displacement of the knee joint.
It happens that the pain accompanying a fracture of the medial condyle of the tibia is completely inconsistent with the complexity of the injury. In this case, it is important to carefully feel the area of damage (palpate the leg). It is important for the specialist what sensations the victim will experience during the process of applying force to specific points.
It is easy to find out the nature of the fracture yourself by pressing just a little on or near the knee joint. Unpleasant sensations will indicate the need for an urgent visit to a medical facility.
The injury is characterized by such a sign as hemarthrosis, which has reached a large size. The joint can increase noticeably in volume, because proper blood circulation is disrupted.
Having noted this, the specialist necessarily directs the patient to undergo a puncture. Puncture is the best procedure for removing blood accumulated in the joint tissues.
Puncture
The first step in case of a fracture without displacement of the fragments is a puncture, through which the effusion and blood located in the joint cavity are removed. After this, a small amount of novocaine solution is injected into the joint cavity, then the joint needs to be immobilized with a plaster cast. Having previously bent the knee joint by 5-10 degrees, the limb is immobilized with a plaster cast.
The application period is about 2-3 months, after which physical therapy classes are necessary as rehabilitation. It is important for the rehabilitation period to start training the thigh muscles. This is done literally 2-3 days after applying the bandage by raising the limb. Later, after about 7 to 10 days, movement on crutches is allowed; it is very important that there is no load on the joint.
Therapeutic measures for fractures with displacement of bone fragments may be different, but initially reposition is required, the return of displaced structures to their normal, anatomical position:
- Having determined the severity and type of fracture, the specialist performs manual reduction under anesthesia, fixes the upper part of the limb, manipulating the lower one. After which an immobilizing plaster cast is applied for the required period.
- The doctor may also decide to treat with constant traction if the fragment is displaced by more than 3 mm. This involves slowly reducing the fragments by applying a special splint to the limb and using a weight system. After a few weeks, if the reduction is successful, the traction system is changed to a plaster cast.
If conservative methods do not give the desired effect or the fracture is quite complex, surgery is prescribed. Displaced fragments are fixed with bolts during the operation, and fusion also occurs for a long time, after which the screwed in bolts are removed.
Diagnostics
The doctor conducts an external examination of the patient and determines the circumstances of the injury. It is necessary to carefully collect anamnesis and analyze the patient’s complaints. After this, instrumental studies begin.
An x-ray is taken, after which the patient is prescribed arthroscopy. This procedure allows you to diagnose the presence of blood in the joint cavity. To clarify the nature of the fracture and the extent of damage, a computed tomography or magnetic resonance imaging may be necessary.
Patients also undergo general clinical examinations (general blood and urine tests), blood biochemistry, and fluorography. This is necessary to determine the general condition of the patient, which is especially important if surgical treatment is necessary.
Main causes of violation
The causes of a fracture are any strong impact on the joint area, occurring along an axis with rotation (rotation). This is observed in the following situations and deviations:
- fall on straight legs from a height (20%);
- a driver or passengers hitting a car bumper with their knee during an accident (50% of all diagnosed pathologies);
- diseases of the musculoskeletal system;
- changes in the structure of bones and other tissues in old age.
Usually a fracture of the lateral condyle is observed, damage to both is in second place, and only in rare cases is there an injury to the internal one.
What is this fracture?
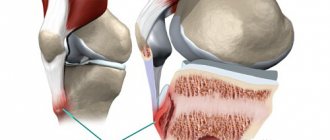
A fracture of the proximal tibia (knee area) includes any type of disruption localized above the tuberosity where the condyles are located. The femur has two of them - medial (inner) and lateral (outer).
The condyle is an osteochondral prominence, with ligamentous apparatus and muscle fibers attached to it. Since it is a more fragile structure than the main bone part, it is most susceptible to fractures. During a fall or impact, a sharp compression or shear occurs with a fracture of one or two condyles.
Fractures can be complete or incomplete. In the first case, there is a crack, crushing or limited depression of the cartilage. With a complete fracture, the condyle (or its fragment) comes off completely. The damage can be combined when ligament rupture or meniscus damage occurs, as well as injury to the intercondylar eminence. Compression and impression fractures are also distinguished separately.
First aid
If you have sustained a fracture of the lateral tibial condyle or any other fracture, the injury should be diagnosed immediately and appropriate treatment initiated. First aid will help the patient wait for qualified specialists to arrive if he is unable to get to the hospital himself. First aid includes:
- Call an ambulance and clarify with a specialist the list of necessary medications allowed for the victim to take in order to relieve pain;
- Anesthesia of the damaged area using analgesic drugs;
- Treating the edges of the wound with an antiseptic; if the wound is open and there is noticeable bone displacement, a mandatory step is to cover the wound with sterile bandages, but tight bandages should not be used;
- Plugging with a sterile cloth will help stop the bleeding in the first couple of days.
If there is no displacement, you need to fix the leg by immobilizing the limb and applying a special splint made from nearby materials.
Recovery period
Improper rehabilitation and the consequences of injury are closely related. Movement disorders and contractures of the knee can be observed in the absence of restorative procedures for the patient.
Rehabilitation should include the following methods:
- physical therapy, starting immediately after removal of the cast. Exercise therapy is aimed at restoring the function of the thigh and lower leg muscles, and includes exercises related to flexion, extension and rotation of the leg joints;
- physiotherapeutic effects (UHF, laser therapy, electrophoresis), improving metabolic processes in tissues and regeneration of damaged structures;
- a balanced diet rich in protein, microelements and vitamins.
Full rehabilitation of the patient can last several months until the motor and support functions of the injured lower limb are completely restored.
Complications
Usually, satisfactory prognosis can be achieved if all medical recommendations are correctly followed. Premature loads provoke subsidence of one of the fragments, which can result in the development of limb deformity and progression of arthrosis. Possible complications:
- Arthrosis;
- Loss of motor function of the knee;
- Nerve damage;
- Infectious infection with an open fracture;
- Angular deformity of the joint;
- Joint instability.
Timely initiation of treatment in full compliance with medical instructions will help to avoid any disappointing consequences and restore the activity of the limb in all cases.
Modern medicine can help choose the most appropriate method of highly effective treatment for condylar fractures.
Rehabilitation
The duration of rehabilitation depends on the severity of the fracture, the speed of reparative processes, the presence of ligament tears, and compression of nerves and blood vessels. In each specific case, only a specialist can determine the duration of recovery.
Light weight bearing, even with a minor fracture of the leg, is allowed only 3-4 weeks after the injury using crutches. Only in this case the possibility of subsidence of the damaged condyle is eliminated.
The patient will be able to lead a normal life only six months after the start of treatment. And in case of severe types of pathology, this period is extended to one year. Physical therapy and physiotherapeutic methods are used to restore knee mobility and strengthen the muscles around it.
It is recommended to take vitamin complexes and calcium supplements during rehabilitation. At this time, it is better to give up bad habits and reduce calorie intake to reduce excess body weight.