2 February 2020
59264
0
4.1 out of 5
A spinal fracture can occur in a person of any gender and age. More often, of course, older people and children encounter it, but healthy men and women in the prime of life are not immune from such a terrible injury. They account for about 2–2.5% of the total number of fractures.
A spinal fracture is a dangerous condition in which the integrity of the vertebral body, intervertebral disc and joints is disrupted. They arise as a result of the action of various mechanical factors, but in any case they require immediate medical attention, as they are fraught with serious complications.
A fracture of the spinal column is always a serious injury, regardless of the type and method of injury. In particularly severe cases, nerve damage occurs, resulting in decreased or complete loss of sensation in the arms, legs, or other parts of the body. Therefore, consultations with a vertebrologist, traumatologist, neurologist, and, if there are indications for surgery, the direct intervention of a neurosurgeon.
Anatomy of the spine
The spine is one of the main organs of the human body, responsible for maintaining it in an upright position. It is formed by 33 vertebrae, between which are intervertebral discs. They are responsible for cushioning bone fragments under static and dynamic loads.
From the back of each vertebra there are arches shaped like a semicircle and forming the spinal canal. It is in it that one of the most important organs of the human body is located - the spinal cord.
The arches have 7 processes:
- 4 articular;
- 2 transverse;
- spinous.
The articular processes of adjacent vertebrae are connected in pairs to each other, thereby forming intervertebral joints. They are entrusted with the function of protection under heavy loads. Thus, openings are formed between 2 adjacent vertebrae, called foraminal. The nerve roots extending from the spinal cord pass through them. Additionally, the bodies, processes and arches are connected by ligaments that provide stability and strength to the entire spine.
Since the spinal cord runs a few millimeters from the spinal column, and its joints are densely penetrated by nerve fibers, spinal fractures are always dangerous. They require not only lengthy and sometimes complex surgical treatment, but also long-term rehabilitation. Moreover, sometimes, despite all the efforts of doctors, such injuries still lead to disability and death.
Causes of spinal fracture
Violation of bone integrity is always a consequence of external mechanical influence. Of course, with calcium metabolism disorders and osteoporosis, the risks increase many times over. But such conditions are only prerequisites, but not causes, of a spinal fracture.
The spine of an adult can withstand up to 400 kg of vertically directed load.
Calcium deficiency in the body can occur in various situations, including:
- rickets (more typical for children);
- pathologies of the parathyroid glands responsible for the production of parathyroid hormone;
- vitamin D deficiency.
Calcium deficiency in the body leads to loosening of bone tissue and a decrease in its strength, i.e., the development of osteoporosis. But direct spinal injury is most often a consequence of:
- car accidents;
- accidents at home or at work;
- sports injuries;
- diving in bodies of water with unknown bottom features;
- military actions;
- falling from a height onto your legs, head or buttocks;
- blows;
- metastasis of malignant tumors to the vertebra.
According to statistics, 82% of patients with spinal fractures are men.
Since the cervical spine is very mobile, it is most often affected in an accident. In such cases they talk about the so-called “whiplash injury”. That is, during a sharp impact or braking, a person fastened with a seat belt to a car seat remains motionless, but the head continues to move forward by inertia, and then sharply leans back. This provokes crushing of the vertebrae of the cervical region and, much less frequently, the thoracic region.
A little about the structure
Before dealing with fractures of the cervical vertebrae, it will be useful to delve into the anatomy of this part of the spine.
Types of spinal fractures
Spinal fractures are classified according to different criteria. To select the correct treatment strategy, not only the location of the injury is important, but also its characteristics. Depending on the nature of the injury and the number of damaged vertebrae, the following types of fractures are distinguished:
- isolated – damage to only one vertebra is observed;
- multiple – several vertebrae are injured at the same time, which can provoke damage to neighboring ones later;
- fragmentation - lead to the separation of sharp bone fragments and additional injury to soft tissue (the most severe type are burst fractures, accompanied by the splitting of the vertebra into several separate fragments);
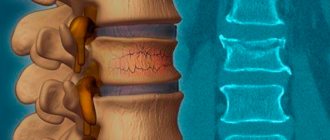
- compression - consist in reducing the height of the vertebral body under compressive influence, i.e. it seems to fall inward;
- stable - the lesion is observed only in the anterior or posterior part of the vertebra, therefore, with such fractures, the spine maintains a stable position;
- unstable - the anterior and posterior sections are simultaneously injured, which creates the preconditions for displacement of the spine;
- compression-fragmentation.
Also, spinal fractures can be complicated by damage to the spinal cord (spinal cord injury) or uncomplicated.
Most often, compression fractures are found, which leads to disruption of the supporting function of the spine and its deformation.
All spinal fractures are classified according to the severity of the deformation of the bone elements. Accordingly, there are 3 degrees of injury:
- 1st degree - the mildest injury, which in most cases can be successfully treated conservatively and rarely leads to complications;
- 2nd degree - more serious damage (with a compression fracture, the height of the vertebra is reduced by less than half);
- 3rd degree – severe injury with a high risk of developing neurological complications (with a compression fracture, the height of the vertebra decreases by more than 50%).
Cervical region
The cervical spine is formed by 7 vertebrae. They are the smallest of all, but protect the most important part of the spinal cord. Moreover, the first 2 have significant differences in anatomy from the others.
The first cervical vertebra (atlas) is ring-shaped and is located just below the occipital bone. A characteristic feature is the absence of an intervertebral disc between them. Since there is no natural shock absorber, the pressure on the skull and in the opposite direction is fully transmitted.
Therefore, when falling on the head, the occipital bone wedges into the ring-shaped vertebra and breaks its anterior and building arches. This injury is called a burst fracture. This is accompanied by severe pain in the back of the head and upper neck.
In almost half of cases, a fracture of the atlas leads to damage to the spinal cord. Sometimes this is accompanied by injury to the medulla oblongata and fracture of the underlying vertebrae. The occurrence of disorders in the spinal cord is indicated by a decrease in sensitivity or even a lack of mobility of the arms and legs. If the medulla oblongata is also affected, this leads to disturbances in breathing and heart function, which can lead to the death of the patient.
The second cervical vertebra or axis is also ring-shaped, but it is additionally equipped with a massive bone growth called the axis tooth. It is designed to fix the atlas, and it is this protrusion that tends to break when the neck is sharply bent. In such cases, the severity of symptoms depends on the amount of displacement of the axis tooth:
- slight discomfort when turning the head (grade I);
- neurological disorders of varying severity from mild changes in sensitivity to paralysis (II degree);
- serious spinal cord injuries, often incompatible with life (III degree).
An axis fracture may also occur. This leads to a displacement of the atlas, often forward, less often to the side or back, which is accompanied by pain in the neck and back of the head that intensifies with movement. In this case, the head takes a forced position, and the person tries to support it with his hands. Injuries like these are typically typical in car accidents in which a person hits the dashboard or windshield.
As for the remaining 5 cervical vertebrae, their fractures are usually compression fractures. This is associated with pain and limited mobility of the neck, and severe muscle tension. But with injuries that lead to ligament rupture, the likelihood of spinal cord damage increases significantly.
Thus, fracture of the vertebrae of the cervical spine is a special category of injuries. Patients with this diagnosis require especially careful care, since the risk of complications that are dangerous to health and life is greatest.
The cervical spine accounts for about 10% of all cases of fractures.
To provide rest to the spine and create favorable conditions for recovery, the neck is immobilized. For this, a Shants collar is usually used. It is recommended to wear it for at least 2 months.
Recovery after a fracture of the cervical vertebrae is especially long.
Thoracic region
The thoracic spine is represented by 12 vertebrae. XI and XII are most often affected, and the number of compression fractures significantly exceeds the number of fragment fractures.
Injuries to the thoracic spine are accompanied by:
- impaired sensitivity and mobility of the chest and arms, sometimes legs;
- pain in the spine, which can periodically radiate to the heart area;
- the occurrence of pain when breathing.
Thoracic fractures occur in 40% of patients with such injuries.
Lumbar
There are only 5 vertebrae in the lumbar spine. These are the largest fragments of the spine, below which is located the sacrum formed by 5 vertebrae fused together.
Fractures of the lumbar spine account for approximately half of all cases.
With injuries to this department, the following is observed:
- pain during palpation, bending, turning the body, sometimes encircling;
- decreased muscle strength or even paralysis of the legs;
- abdominal pain, feeling of bloating;
- impaired sensitivity and decreased strength of leg reflexes;
- sometimes cramps;
- disturbances in the functioning of the urinary system, in particular urinary retention or, conversely, uncontrolled urinary diversion;
- erectile dysfunction or decreased sensitivity of the genital organs (in men).
Spinal fracture in children and the elderly
It is children and elderly people, due to their metabolic characteristics, who most often have calcium deficiency in the body. Therefore, in order to damage the spine, a fairly weak mechanical effect is sufficient, which in another case would not lead to any undesirable consequences.
Since most often the damage to the spine is not very extensive, patients usually notice only moderate pain in the area where the blow was received. An outside observer may notice the formation of a kind of hump in the projection of the broken vertebra. Only in rare cases is the injury accompanied by severe pain and other symptoms of a fracture. Therefore, patients in these groups seek medical help much later than they should.
Damage classification
There are several options for how to divide a cervical vertebrae fracture. Below are the most frequently used classifications in practical healthcare.
- The nature:
- compression, as a result of compression of the vertebral body;
- splintered, with the presence of fragments;
- fracture-dislocation;
- fracture of the arches.
In the penultimate variant, along with dislocation of the articular processes, a fracture of the body or arches is observed.
- Presence of complications:
- complicated;
- uncomplicated.
This means with or without spinal cord damage.
- By localization:
- diver's injury (vertebrae 3 to 7 are damaged, ligaments are torn);
- damage to the first vertebra (Jefferson fracture);
- damage to the second vertebra (hangman's fracture);
- damage to the mole rat (fracture of the spinous processes of the 6th and 7th vertebrae).
Clinical picture
The nature of the symptoms depends on the type of fracture and its location. In the vast majority of cases, immediately at the time of injury, a person feels severe pain in the spine in the projection of the damaged vertebra. Gradually the pain dulls, but does not disappear. Sometimes it radiates to the abdomen and most often gets worse when walking or getting out of bed, but tends to get better when lying down.
Pressing on the spinous processes is painful. In some cases, the gap between them increases or, on the contrary, decreases. But the most typical sign of a spinal fracture is pain at the site of injury when gentle pressure is applied to the head. However, you cannot try to diagnose a fracture yourself in this way. If there is an unstable fracture, pressure on the spine can cause displacement of fragments and characteristic complications.
Sometimes you can notice a smoothing of the outlines of the dorsal groove of the spine, as well as slight swelling and a slight protrusion in the projection of the lesion.
Almost half of women over 80 years of age show signs of an old compression fracture of the spine on x-rays. Moreover, the overwhelming majority of them were absolutely sure that back pain was a consequence of age-related changes.
A spinal fracture may also be accompanied by:
- nausea;
- vomiting;
- numbness of hands and feet;
- headache;
- difficulty turning the body;
- constant tension in the back muscles;
- decreased growth;
- the formation of a hump or an unnatural arch of the back;
- ascending edema, cardiac dysfunction;
- dysfunction of the pelvic organs.
If the thoracic or lumbar spine is fractured, breathing may be difficult and pain may increase with a deep breath or cough.
If the injury is accompanied by damage to the nerves or spinal cord, the clinical picture characteristic of an uncomplicated fracture is supplemented by:
- impaired sensitivity of the limbs;
- paresis or paralysis;
- dysfunction of the pelvic organs (involuntary release of urine or feces).
Most often, fragmentation and severe compression fractures provoke the appearance of neurological symptoms. But if several vertebrae are injured at the same time, a combination of symptoms of their damage is observed.
What is the danger of pathology?
It is important to understand that any pathology that affects a vital anatomical formation, with an illiterate approach or lack of appropriate therapy, can result in dire consequences for a person. Timely treatment and rehabilitation after a compression fracture of the lumbar, thoracic or cervical spine will help to avoid all negative complications. We will talk about them further.
The spinal system serves as a container for the most important component of the central nervous system - the spinal cord. Thanks to the spinal substance, musculoskeletal functions are ensured, in other words, the overall ability to move and maintain a stable body position.
The spinal canal, its nerve roots, arterial and venous vessels affected by pathological pathogenesis, which is more often observed with compression-comminuted fractures, with traumatic excesses with the formation of wedge-shaped deformities and instability of elements, is not a joke. The degree of damage to the spinal cord can vary - from concussions, compression and contusions, to its complete rupture.
The worst thing that a neglected clinic can threaten is partial or complete paralysis of the body.
In addition, without urgent medical care and rehabilitation after compression fractures in the spine, secondary degenerative and neurological diseases develop, which will be very difficult to combat. These include:
- segmental instability in the damaged area;
- osteochondrosis and intervertebral hernia;
- kyphosis of the spinal column, or non-physiological curvature;
- radiculopathy, paresis and other neurogenic disorders;
- spinal canal stenosis;
- vascular malformations and development of hematoma in the epidural space;
- chronic pain, paresthesia;
- persistent movement disorders;
- dysfunction of the pelvic organs.
Therefore, do not risk feeling discomfort and pain in your back, especially if they appeared immediately or after a certain time after an injury or unsuccessful movement. You can’t hesitate here, believing that nothing serious has happened. It is better to be examined once and make sure that everything is really in order, than to ignore a dangerous problem and pay for your indifference at the cost of your own ability to work.
Diagnostics
It is not difficult to detect a spinal fracture. After examining the patient, a vertebrologist can with a high degree of probability assume its presence, and in order to confirm the diagnosis, the patient is prescribed:
- X-ray in anteroposterior and lateral projections;
- CT;
- MRI.
To diagnose an atlas fracture, x-rays are taken through the mouth.
Often, spinal fractures are combined with damage to the surrounding ligaments, muscles and intervertebral discs. And a grade I fracture of the axis tooth is not always visible on x-rays. Therefore, in controversial cases, only X-rays are not enough; it is then that a more informative study, CT, is indicated. Also, an indication for performing a computed tomography is a suspicion of an unstable fracture.
If the patient has neurological disorders, an MRI is required. The method allows you to detect damage to the nerve roots and the spinal cord itself. During the examination, herniated intervertebral discs are often discovered.
Neck fracture: indirect signs
Indirect symptoms of a cervical fracture include:
- Excessive strain on muscles;
- state of nausea;
- dizziness;
- mobility impairment.
Dizziness is one of the possible indirect symptoms of a neck fracture.
If the patient's breathing becomes rapid and intermittent, such symptoms indicate a serious danger to the victim's life.
Conservative treatment of a spinal fracture
For mild, uncomplicated fractures, conservative treatment is possible. It is prescribed by a vertebrologist or traumatologist. For each patient, the nature and duration of the course of treatment is selected individually. It is indicated only for first-degree fractures without vertebral displacement.
From the first days of therapy, patients are prescribed:
- drug therapy;
- immobilization;
- gentle regime;
- physiotherapy.
Sometimes patients are shown skeletal traction. It is performed under X-ray control in order to increase the space between the vertebral bodies, which creates favorable preconditions for restoring their normal position. After this, the spine is fixed by applying a plaster corset.
Additionally, the following may be prescribed:
- static therapeutic exercises;
- electromyostimulation;
- water procedures.
Drug therapy
Patients are prescribed a complex of medications aimed at eliminating pain, accelerating the straightening of the vertebral body (with a compression fracture) and activating recovery processes. This:
- painkillers (in the first days after injury and severe pain, narcotic drugs can be used, from which they subsequently switch to NSAIDs);
- novocaine injections;
- chondroprotectors;
- calcium supplements and vitamin D;
- antibiotics;
- nootropics;
- vasodilators;
- cholinomimetics;
- corticosteroids;
- cyclooxygenase-1 blockers and others.
Chondroprotectors and calcium supplements together with vitamin D should be used for the longest time. But while mineral supplements have long proven their effectiveness, chondroprotectors do not have a convincing evidence base.
Immobilization
The patient's spine is immediately immobilized after skeletal traction is performed. Fixation of the damaged segment of the spine with a reclinator, rigid orthopedic or plaster corset reduces the load on it, reduces the risk of complications and creates favorable conditions for restoring bone integrity.
Wearing an orthopedic corset or Shants collar is usually indicated for up to 4 months. And with compression fractures, patients are quickly allowed to walk independently.
Gentle mode
A gentle regimen with limited physical activity is prescribed for up to 12–14 weeks. At this time, it is especially important to avoid stress on the spinal column. It is forbidden to sit, lift weights, make sharp turns of the body, or lean forward.
Periodically, to monitor the quality of vertebral fusion, x-rays of the affected part of the spine are taken. Additionally, the condition of the lungs, muscles and nerve conduction is assessed through:
- chest x-ray;
- electromyography;
- electroneurography;
- neurological examination with assessment of reflexes and autonomic reactions.
Physiotherapy
Physiotherapeutic procedures are recommended for patients with spinal fractures to reduce pain:
- UV radiation above the injury site;
- UHF low-thermal intensity;
- inductometry in the fracture area;
- Sollux;
- ultrasound therapy;
- electrophoresis with calcium and phosphorus;
- paraffin, ozokerite and mud applications.
After immobilization, the procedures are carried out through a cast. As a rule, a course of 10–12 sessions is prescribed, each lasting 10–15 minutes.
Surgical methods (operation) for spinal fracture
Conservative therapy is not always capable of restoring normal vertebral anatomy and eliminating the consequences of injury. In such situations, surgical treatment is indicated for patients. Also indications for its implementation are:
- unstable vertebral fractures;
- comminuted fractures;
- presence of neurological symptoms.
The tactics and type of surgical intervention are selected individually by the neurosurgeon depending on the nature of the fracture and the results of the studies performed. Traditionally, vertebroplasty or kyphoplasty is performed to eliminate the consequences of spinal column injury. These techniques are highly effective and safe, making them the best option for surgical treatment of spinal fractures.
In case of severe injuries, fixing operations are performed, during which the following are installed:
- Z-plates;
- dorsal metal structures, in particular transpedicular fixators;
- laminar flow contractors;
- grids;
- Luque systems.
If it is impossible to restore normal anatomy with these means, patients are indicated for laminectomy and installation of autografts or artificial implants. The choice of treatment method for a complex spinal fracture depends not only on its location, but also on the degree of spinal canal stenosis, the characteristics of neurological disorders and how much time has passed since the injury.
Vertebroplasty
Vertebroplasty is a microsurgical intervention that involves connecting and increasing the strength of the vertebra by introducing bone cement into it using a puncture needle. It fills all the pores of spongy bone tissue and glues together scattered bone fragments into a single whole. In more than 85% of cases, this leads to immediate elimination of the defect, and in the remaining 15%, an increase in positive changes was observed within several days after surgery.
Bone cement is a composite material created on the basis of polymethyl methacrylate and has high viscosity, biomechanical strength and maximum biocompatibility.
The procedure is performed under local anesthesia and does not require prolonged hospitalization. Its essence is as follows:
- the skin of the back in the area where the puncture needle is inserted is treated with an antiseptic and marked;
- a needle is inserted into the injured vertebra under X-ray control;
- prepare bone cement and immediately inject it through a puncture needle, filling all intravertebral structures (the quality of filling is controlled using X-rays);
- remove the instrument, treat the wound with an antiseptic and cover it with a sterile bandage.
The bone cement is prepared immediately before insertion as it takes 10 minutes to fully harden. To do this, use a special mixer to mix the liquid monomer with the powdered polymer. This is accompanied by an active chemical polymerization reaction, which occurs with the release of thermal energy for 8–10 minutes. Then the mass hardens, as a result of which the treated vertebra acquires high strength and hardness, which is an excellent prevention of subsequent fractures.
Because bone cement contains the antibiotic gentamicin or vancomycin, vertebroplasty carries minimal risk of postoperative infectious complications. And the presence of barium sulfate in its composition provides complete control over the completeness of filling the vertebra that has sagged as a result of a compression fracture at each stage of the surgical intervention.
But vertebroplasty cannot be performed if:
- reduction in height by more than 70%;
- allergies to bone cement components;
- metastases;
- severe neurological symptoms caused by severe compression of the nerves in the area of the affected vertebra.
Kyphoplasty
Kyphoplasty is a microsurgical intervention that has much in common with vertebroplasty, but is characterized by greater safety and capabilities. It is especially effective for fractures of the thoracic and lumbar spine resulting from osteoporosis.
Kyphoplasty is effective even with:
- compression fractures accompanied by a decrease in vertebral height by more than 70%;
- osteoclastic processes in the vertebral bodies.
The operation is carried out in 2 stages:
- Installation of a balloon that returns the vertebrae to their normal position by injecting the required volume of saline solution mixed with an X-ray contrast agent into it.
- Introduction of special bone cement based on polymethyl methacrylate, which secures the bone structures in the balloon-formed state.
The surgical intervention is performed under general anesthesia through an incision up to 1 cm in size. All manipulations from the introduction of a hollow cannula to its removal from the body are performed under X-ray control, which allows you to fully control the process of restoring the anatomy of the spine.
Improvement in condition is observed immediately after completion of the operation. At the same time, kyphoplasty eliminates the risk of kyphotic deformation, especially characteristic of elderly patients, and, accordingly, the occurrence of disturbances in the functioning of internal organs.
Unlike vertebroplasty, the risk of spreading of the injected bone cement beyond the vertebra is reduced to almost 0. In addition, it allows you to restore the normal size of the compressed vertebra and eliminate the likelihood of developing kyphosis. Therefore, it is a more reliable method of treatment, but also has a higher cost.
Transpedicular fixation
In case of complex, especially fragmented and unstable fractures, it is often necessary to rigidly fix the vertebra in the desired position. It is for this purpose that the transpedicular fixation method is used.
The operation is quite traumatic and involves stabilizing the vertebrae with special titanium screws that are screwed through their pedicles. Each vertebra has its own screw insertion point at the intersection of the transverse process with the superior articular process.
Since spinal fractures often affect intervertebral discs, they must be removed in such situations. To fill the resulting space between the vertebral bodies, either special artificial cages or autografts are used and complete interbody fusion is achieved.
Transpedicular fixation or TFT is performed under general anesthesia and under X-ray control (usually image intensifier or CT). Briefly, its essence can be expressed as follows:
- making an incision in the projection of the fracture;
- separation of the spinous processes and vertebral arches from soft tissues;
- perforation of the transverse and articular processes with a special probe;
- installation of screws of the required type and size;
- combining the screws with springy rods, ensuring uniform distribution of the load over the entire structure;
- suturing.
Since titanium has high strength indicators, the installation of screws made from it ensures the resistance of the entire assembled structure to any deforming loads, and the presence of surface caps prevents its distortion.
Transpedicular fixation has a number of significant advantages in the treatment of spinal fractures, since by installing only one small structure it solves the problem of moving the vertebra to an anatomically correct position and at the same time locks only a small area of the spine. It is associated with a low risk of damage to nerves and blood vessels and, despite a fairly serious intervention in the body, provides early mobilization of the patient. At the same time, during the operation, the neurosurgeon has the opportunity to decompress the neural structures and ensure the elimination of the symptoms accompanying their compression, provided that the nerves are still viable.
The method cannot be used only if there are serious intraoperative risks associated with the patient’s concomitant diseases. Also, its use is associated with significant difficulties when it is necessary to fix the upper thoracic vertebrae, since they are small.
Laminectomy
Laminectomy is the most traumatic operation performed for spinal fractures. But it provides good access to the damaged vertebra and allows you to solve a large number of problems at once.
The method involves making a large incision and removing the spinous processes and vertebral arches. As a result, the neurosurgeon can release the nerve roots of the spinal cord compressed by bone fragments and normalize the innervation of the corresponding parts of the body.
Sometimes the entire vertebra and intervertebral disc are removed during surgery. In such cases, they try to replace it with an artificial endoprosthesis or use the patient’s own bones to preserve the supporting function.
The disadvantage of this method is the long and difficult recovery period, as well as the formation of noticeable postoperative scars.
Rehabilitation
Recovery from a spinal fracture is a long and often painful process. But an integrated approach to this issue ensures the return of lost functions partially or fully. There is a rehabilitation period both after surgery and with conservative treatment. In both cases, it is equally important to follow the doctor’s recommendations and not neglect exercise.
After surgical treatment, in most cases, patients are discharged from the hospital within 3–5 days. At first, they are advised to remain in bed to minimize vertical loads on the spine. Otherwise, there is a possibility of resorption of the damaged vertebral body and deformation of the spinal canal. This leads to the development of severe neurotic disorders, which in medicine is called Kümmel's disease.
In the future, patients are recommended to:
- Exercise therapy – performing a specific set of exercises under the guidance of a specialist, and then independently, helps strengthen the muscle corset and reduce the load on the spine. In the first week, breathing exercises and joint exercises are usually recommended, but gradually the complex becomes more complex to achieve optimal results.
- Reflexotherapy – impact on biologically active points leads to increased blood circulation and activation of regeneration processes of damaged tissues.
- Manual therapy is indicated 2 months after the start of rehabilitation and only if the dynamics are positive. Sessions should be conducted only by a highly qualified specialist who accurately understands the peculiarities of the body’s recovery after such severe injuries.
The final stage of rehabilitation is sanatorium-resort treatment. Sometimes cyclic rehabilitation courses are indicated for maximum recovery in severe cases.
With competent behavior during the recovery period, patients with 1st degree fractures are completely rehabilitated in 1–8 months, with 2nd degree fractures – in 10–12 months. If a person had a third-degree spinal injury, the prognosis depends on which part was damaged and what other structures were damaged. In such situations, it may take 1.5 to 2 years before returning to a normal lifestyle, and in especially severe cases, even the most experienced doctors are not able to prevent the onset of paralysis.
First aid measures
First aid for neck fractures is very important and affects the outcome of further treatment, as well as the rehabilitation period. As a result of the injury, the patient's vertebrae have become misaligned and the patient may suffocate due to lack of air.
To relieve discomfort and allow the respiratory system to function, the person must be placed on a flat, hard surface. During transportation, the neck and head should be securely secured to prevent negative consequences.
If the person is in severe pain, painkillers may be given, but without turning the head. Tablets can be prescribed to a patient only in the absence of a violation of the swallowing reflex. When swelling occurs after injury, first aid is to gently move the patient onto their stomach. This is the only time the victim's body is allowed to rotate.
Possible complications
Spinal fractures often lead to complications, especially if proper treatment is not carried out. Thus, compression fractures with a decrease in vertebral height by more than 50% can lead to their increased mobility, which is called segmental instability. This condition is characterized by:
- the appearance of constant pain;
- rapid degenerative changes in the affected spinal motion segment;
- damage to nerve structures, which leads to the appearance of typical symptoms and their persistence (paresis, paralysis of the limbs, convulsions, sensory disturbances, problems in the functioning of internal organs).
In people of the older age group, the formation of the so-called senile hump is possible, which becomes a consequence of kyphotic deformity. This also leads to constant pain of varying intensity. It is these that people often attribute to age-related changes and do not even suspect the presence of a spinal injury.
But the most severe complication of a spinal fracture is rupture or compression of the nerve roots of the spinal cord and itself. This can happen either immediately at the time of injury or subsequently against the background of degenerative changes. Often in such cases, the blood vessels that supply the spinal cord are damaged and compressive myelopathy is observed. This is accompanied by increasing neurological disorders, which can only be eliminated through surgery.
Thus, a spinal fracture is a serious injury that can leave a heavy imprint on a person’s future life or even take it away. But immediate consultation with a doctor, a responsible approach to treatment and subsequent rehabilitation allows you to avoid the development of undesirable consequences or minimize them.