Do you feel like your little one's legs or arms are growing slowly? He may have Ollier's disease. This is a disease in which abnormalities in the development of the bone skeleton occur, that is, its dysplasia. Other names for the disease mentioned are multiple chondromatosis of bone, unilateral chondromatosis, or dyschondroplasia of bone. The disease received its main name from the name of the Lyon surgeon Ollier. He discovered and described the disease using X-rays in 1899.
What is Ollier disease
This disease refers to anomalies in the development of the bone skeleton, which include many diseases, including hip dysplasia, which is well known to many mothers of babies.
The disease most often manifests itself in childhood, which is why it was previously thought that it was a disease of children. It has now been proven that the pathology can also debut in adults (signs can appear even at the age of 20-40 years). This is a congenital pathology, but it is discovered after some time - in early childhood or adolescence - that is, during intensive growth, when bone deformations and / or abnormal development of the arms and legs become obvious.
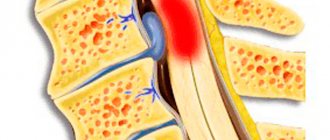
With Ollier's disease, cartilage growths appear in the metaphyses of the long tubular bones of the limbs. The disease develops mainly in the bones, cartilage and joints of the arms and legs, in particular in the feet and hands, as well as in the pelvic bones, but it also occurs in the ribs, sternum or skull.
The growths, or enchondromas, make the outer layer of bone thin and fragile. Essentially, these are benign tumors that can develop into malignant ones (for example, chondrosarcomas). Fortunately, this happens extremely rarely.
During puberty, the growths stabilize and are replaced by bone.
So, Ollier's disease is a severe hereditary disease, ossification of the cartilaginous skeleton, in which thickening of the metaphyses (necks of tubular bones) also occurs. The cause of its occurrence is still unknown. In some cases, it is of an autosomal dominant genetic nature.
Diseases similar to dyschondroplasia are the rare Maffucci and Proteus syndromes. In the first case, in addition to benign cartilaginous growths and skeletal deformations, hemangiomas are formed on the skin - dark red spots of irregular shape, consisting of blood vessels. In the second, benign tumors develop in various parts of the body.
Pathogens
The causative agents of Lyme disease are several species of human pathogenic borrelia - Borrelia burgdorferi, Borrelia garinii and Borrelia afzelii. Borrelia are microaerophiles and, like other gram-negative spirochetes, are extremely demanding on cultivation conditions. Infections caused by Borrelia burgdorferi most often present with arthritis (especially in North America, where it is the only causative agent of borreliosis), while B. garinii is more likely to cause neurological disorders and B. afzelii is more likely to cause chronic skin diseases. All three pathogens cause erythema migrans.
Who is susceptible to the disease
Chondromatosis of the bones was previously thought to be rare. But now, when X-ray examination is carried out quite widely, it turned out that it cannot be called a rarity. If 20 years ago 30 cases were described, now there are twice as many.
It is usually impossible to determine the exact onset if regular dynamic X-ray examinations have not been carried out since birth, especially in early childhood and intrauterine development, when, in fact, Ollier’s disease occurs. By the way, this disease is detected in girls almost twice as often as in boys.
Diagnostic measures
The final diagnosis of dyschondroplasia is established on the basis of an external examination of the patient, collection of anamnestic data and an x-ray examination. If the development of Ollier's disease is suspected, extended radiography (segmental) of all areas with suspected endochondroma formation is recommended.
It is important to consider that today there are no effective methods for eliminating the symptoms of the disease in children (during the period of bone tissue growth). As a rule, after surgical removal of the changed area, relapses are observed.
An x-ray reveals swollen and thickened metaphyses, which are shaped like a club, and the diaphyses are curved depending on the degree of progression of the disease. Locally, there is no bone tissue in the chondromatous nodes, and these areas are lighter in the image.
An x-ray of a patient with Ollier's disease allows for a comparative description of the hands. On the right hand there are lytic changes in almost all bones, as well as destruction of their phalanges with foci of calcification, which indicates severe multiple lesions
With thickening of the epiphysis, thinning of the tissues is observed, their elevated position above the foci of inflammation of the cortical layer and the absence of a periosteal reaction. When dyschondroplasia occurs with damage to the scapular region, the cartilaginous focus is located at the periphery, and in the central part of the bone its normal shape is preserved. When rib tissue is involved in the inflammatory process, the image shows the localization of the anterior end of the rib in the absence of characteristic swelling.
Corrective intervention is also ineffective, which is explained by the immature structure of the bone tissue, so the main emphasis is on the use of orthopedic devices and systematic examinations of the child until the period when the skeletal bones stop growing. After this, excision of the affected area is performed and subsequent application of the Ilizarov apparatus.
Symptoms of the disease
In order not to miss signs of the disease, parents should be wary if their child:
- some areas of the limb/limbs are delayed in development;
- asymmetry and shortening are noted in them;
- lameness is observed;
- there is a pelvic distortion;
- there are curvatures of the joints of the valgus or varus type.
All these factors make it possible to assume that the child has Ollier disease.
The disease does not always appear immediately at birth, but already at the age of 1-4 years you can notice that the child’s legs or arms are growing more slowly than expected. This is the main symptom of the disease that cannot be ignored. Otherwise, the baby is developing normally, despite the fact that he was diagnosed with Ollier disease.
Dyschondroplasia most often affects one limb, however, cases of damage to both are not uncommon. If the disease affects the legs, the child will be short due to their shortening. Bone growth is especially severely delayed if the pathological process began very early. The deformities are painful and progress slowly. The limb affected by the disease becomes shorter, thicker, the gait changes, and lameness is observed. Varus or valgus deformity of the knee (less commonly, the proximal end of the thigh or foot), and scoliosis of the spine may be observed. Muscle atrophy is not present in this disease.
The phalanges, metatarsals and, in some cases, metacarpal bones undergo major changes. They are shortened, widened, awkward and contain many cartilaginous enlightenments.
People suffering from Ollier disease are susceptible to fractures because their bone tissue does not develop properly as a result of the disease. However, fractures most often heal without problems.
Epidemiology
The natural hosts of Borrelia in nature are wild animals (rodents, birds, deer), which feed ticks of the genus Ixodes - carriers of Borrelia. During blood sucking, borrelia enter the tick's intestines, where they multiply and are excreted in feces. Despite the high level of infection of ticks, the possibility of infection through a bite is not always realized, because borrelia are contained in the salivary glands in small quantities or are absent altogether.
In natural foci, the circulation of the pathogen occurs as follows: ticks → wild animals → ticks. It is possible that domestic animals - goats, sheep, cows - may be involved in the epidemiological chain. The likelihood of other carriers of Borrelia, such as horse flies, is being studied. A person becomes infected with Lyme disease in natural foci. Natural foci of Lyme disease are found mainly in forest landscapes of the temperate climate zone. In recent years, it has been established that the area of distribution of tick-borne borreliosis coincides with tick-borne encephalitis, and the disease is registered throughout the Russian Federation. However, the incidence of Lyme disease is 2-4 times higher than tick-borne encephalitis, and it occupies one of the first places among natural focal zoonoses. Tick-borne borreliosis is widespread in Europe, Asia, and America. In Russia, borreliosis is widespread in the forest and forest-steppe zones from Kaliningrad to Sakhalin. In European Russia, borreliosis is the most common tick-borne infection.
The risk of getting borreliosis after a tick bite is much higher than tick-borne encephalitis. Natural foci of tick-borne borreliosis coincide with the range of ixodid ticks. The incidence of borreliosis is seasonal and coincides with the activity of ticks. The first patients with tick bites are usually registered in March-April. The latter, in the presence of warm weather, are recorded even in October. Peak activity occurs in May-June. The percentage of ticks infected with borreliosis differs in different regions. A tick can simultaneously be infected with Borrelia, tick-borne encephalitis virus and other pathogens. Therefore, the development of a mixed infection is possible.
Transmission of the infection occurs transmissibly through a tick bite (inoculation), although the possibility of infection cannot be ruled out when tick feces come into contact with the skin, followed by rubbing them in when scratching (contamination). In case of a tick rupture, due to improper removal? the pathogen may enter the wound. The nutritional route of infection through consumption of raw goat or cow milk is discussed.
The main risk groups are workers of forestry farms, timber industry enterprises, hunters, foresters and residents of forested areas.
The carriers of Borrelia are ticks of the genus Ixodes, in our country and Europe - I. ricinus and I. persulcatus, in America - I. pacificus and I. scapularis. The life cycle of these ticks (larva - nymph - adult) lasts an average of three years. Ticks become infected from numerous rodents, as well as hares, hedgehogs, birds, etc. Ticks live in grasses, ferns and low shrubs.
Differential diagnosis
Differential diagnosis for Ollier's disease, in fact, is not needed after an X-ray examination, since the picture of chondromatosis is very specific. However, each case is individual, and the set of painful signs is practically not repeated, so doctors should exclude a number of similar diseases.
X-ray excludes atypical chondrodystrophy, hemihypertrophy or hemiatrophy of bones, rachitic deformities and some other diseases. Also, thanks to x-rays, Recklinghausen's disease, which can usually be confused with Ollier's disease, is excluded. The main principle is that it is necessary to take an x-ray of the entire skeleton, and not part of it.
conclusions
Since no single protocol has been developed for the choice of treatment method for children and adolescents with tumors and tumor-like diseases, the course of which was complicated by pathological fractures, each case requires a differentiated approach to treatment and depends on the nature, location of the fracture, as well as the age of the patient and the nosological affiliation of the underlying disease, which must be confirmed morphologically.
Information about authors
For contacts:
Snetkov A.I. — email
Principles of treatment
Dyschondroplasia currently, unfortunately, has no methods of rational treatment. Unlike, for example, a disease such as hip dysplasia, chondromatosis can only be treated by surgical correction of the deformity. In some cases, artificial endoprosthesis replacement is indicated. The rest of the treatment that the patient should receive is symptomatic and supportive.
Surgical intervention is indicated mainly for adults, since, according to modern observations, no lasting results were obtained with surgical correction at school age, which means that it makes sense to carry out surgical treatment only for mature deformities, but not for dynamic ones. However, in case of severe lesions, surgical intervention is also possible for children, especially when it comes to fingers, which are significantly bent due to Ollier's disease.
The disease requires the maintenance of joints and bones: patients are advised to wear orthopedic shoes, use an orthopedic apparatus and other devices to secure the joints. Patients must necessarily engage in physical therapy exercises designed specifically for this pathology.
Gymnastics and exercises on special machines are also useful. This helps restore muscle tone and strengthen ligaments.
results
The results of treatment were monitored over a period of 1 to 9 years. The effectiveness of treatment was assessed taking into account oncological and orthopedic criteria. The effectiveness criteria were the absence of complaints, relapse of the disease, signs of consolidation of the pathological fracture, and function of the operated limb.
All patients underwent safe osteoplastic surgery, only in 1 case no surgical treatment was performed, since repair of the pathological focus was recorded after healing of the fracture against the background of the cyst. The period of immobilization in a plaster cast was 6 weeks. In situations with other patients, surgical treatment was necessary. Considering the absence of displacement or the presence of slight displacement of bone fragments and the nosological affiliation of the underlying disease, fixation with plaster casts in 21 cases was the first stage of treatment. Fixation mainly lasted 1 month from the moment of injury, thereby consolidating the fracture, which ensured the creation of more favorable conditions for surgical treatment. In case of significant displacement, the first stage was trephine biopsy to verify the diagnosis and closed reposition to eliminate gross displacement. After which the affected limb was fixed with a plaster cast or a skeletal traction system was applied. After morphological verification of the diagnosis, patients underwent open reduction of the fracture, removal of pathological tissue, alloplasty and, if necessary, metal osteosynthesis. Patients operated on without metal osteosynthesis were treated with unloading and fixation of the affected limb with a plaster cast for 3 months from the date of surgery. Next, the plaster cast was removed and the development of movements in the joints of the operated limb began. Full weight-bearing was recommended 4 months after surgery. The use of bone osteosynthesis made it possible to abandon the use of external immobilization and begin early activation of the patient, to begin early development of movements in the joints of the operated limb, which in turn helped to reduce the length of hospital treatment and facilitate patient care.
In the presence of a metal fixator, the development of movements in the joints of the affected limb began 1 week after the operation, and full load - after 1 month. In the postoperative period, dynamic observation of all patients who received surgical treatment in the department was carried out. Control radiographs were taken 3, 6, 9 and 12 months after surgery. Consolidation of fractures was observed 2.5–3 months after surgery. The timing of non-organotypic reconstruction of grafts depended on a number of factors: the volume of the post-resection defect, the number, type and type of grafts and nosology of the disease. Autografts were reconstructed most quickly in a period of 8 to 12 months. With the isolated use of Perfoost grafts, the period of reconstruction took on average from 12 to 14 months. In cases of massive alloplasty with extensive bone resections, when superficially demineralized allo-implants were combined with cortical frozen implants, the reconstruction period increased to 18 months.
The timing of removal of metal structures depended on the nosology of the pathological process. In fibrous and osteofibrous dysplasia, taking into account the nature of the disease, metal structures were left in place to prevent the occurrence of deformities and pathological fractures in the long-term postoperative period. In other cases, the metal structures were removed 1.5–2 years after the operation.
The following complications were recorded between 3 and 6 months. In case of bone cysts: in 5 cases - relapse of the underlying disease, in 2 - shortening of the damaged segment, 1 case each - joint contractures and neurological disorders; with fibrous dysplasia: in 1 patient - shortening of the damaged segment; with non-osteogenic fibroma: 2 – joint contractures. In the long-term postoperative period (9–18 months) with fibrous dysplasia, migration of metal structures was noted in 2 cases.
Forecast
According to research, most often by puberty, cartilage tissue is replaced by bone tissue (perhaps this is why cases of the disease are extremely rare in adults). However, in young children the prognosis is less rosy: the deformation, although slowly, progresses. This is precisely why Ollier's disease is dangerous.
The disease manifests itself so individually in each case that it is difficult to clearly assess the overall prognosis. With numerous lesions it is more favorable than in the case of localized single changes. Single deformities lead to shortening of one of the limbs and, consequently, to their asymmetry, especially when it comes to small children. And this can no longer be corrected. Also, with the early development of tumors, the risk of various finger deformities increases.
Classification
There are several options for systematizing Ollier's disease, based on the localization and extent of the pathological process. Taking into account the number of affected bones according to the classification of M.V. Volkov distinguishes between monoosseous (1 bone is affected), oligoosseous (2-3 bones are involved in the process) and polyosseous (areas of embryonic cartilage are found in many bones) variants of the disease. The classification of A.A Arenberg involves the identification of four forms:
- Acroform
. Damage to small bones of the distal extremities (hands, feet) is observed. - Monomelic form
. The bones of the limb and the adjacent bones of the body (pelvis, scapula) have been changed. - One-sided form
. Zones of cartilage in the bones are localized on one side or there is significant unevenness of the lesion with predominant involvement of one half of the body. - Double-sided form
. The most common. Areas of cartilage are found in both halves of the body, usually located asymmetrically.
In the specialized literature there is also a division based on the structural features of embryonic cartilage and its tendency to intensive growth. There are three types of cartilaginous tissue: close in structure to ordinary hyaline cartilage, reminiscent of chondroma (fast-growing, rich in blood vessels, causing destruction of adjacent bone) and occupying an intermediate position between these two options.