Psoriatic arthritis
is a secondary inflammatory disease of the joints with a chronic course. It appears in every 4th patient with psoriasis as a consequence of the underlying disease. Often the inflammatory process affects not only the peripheral joints, but also spreads to the spine, involving ligaments and tendons.
Psoriatic arthritis is a chronic inflammation of the joints, a consequence of psoriasis.
Usually the disease makes itself felt at the age of 25-50 years, but an earlier, juvenile form
, in which the onset of the disease occurs at the age of 9-11 years. By a slight margin, women are more susceptible to psoriatic arthritis.
Although the disease is usually mild to moderate, approximately 10-15% of patients suffer from a disabling form
.
General information
Psoriatic arthritis (PsA) or psoriatic arthropathy is a chronic systemic disease of the musculoskeletal system associated with psoriasis, that is, concomitant with it. Codes for the International Classification of Diseases, 10th revision (ICD-10) - L 40.5, M07.0 - M07.3.
According to statistics, the incidence of PsA is 3–8 per 100,000 population. Inflammatory processes in the joints with psoriasis more often appear in people against the background of existing skin rashes (70% of all patients). But it also happens the other way around, when psoriatic arthritis is the only manifestation of the disease, which significantly complicates timely diagnosis. There are about 15% of such patients; the same number of patients had both skin and joint symptoms.
Diet recommendations
The therapeutic diet for psoriatic arthritis involves eating plenty of fruits and vegetables. The following options are especially recommended:
- sea buckthorn, raisins and rowan;
- peaches, pineapples and kiwi;
- lemon and lime;
- directly pressed juices;
- baked apples;
- hazelnuts and almonds;
- dates;
- herbal teas;
- steamed fish;
- celery, spinach and sorrel;
- turkey and lamb;
- dairy products.
During treatment, you must refrain from salt, pepper, concentrated fish and meat broths, as well as alcoholic beverages.
Why and how the disease develops
The causes of psoriasis have not been fully established. It is believed that the immune system and hereditary predisposition play a major role in the development of psoriatic arthritis. It has been established that about 40% of patients with PsA have close relatives suffering from psoriasis.
Under the influence of any trigger factors (nervous stress, infection, hypothermia, alcohol abuse, etc.), genetically predisposed individuals experience a malfunction of the immune system. Normally, immune cells produce information molecules—cytokines—that regulate inflammatory reactions. A malfunction of the immune system leads to the fact that the normal ratio of cytokines that support and suppress inflammation is disrupted, a cytokine storm develops, and inflammation becomes uncontrollable.
Genetic predisposition manifests itself in the presence of certain antigens in the body. Thus, in the presence of the B38 antigen, psoriatic arthritis rapidly progresses with the development of a destructive process that destroys the articular surface. The presence of B17 and Cw6 antigens indicates the possible involvement of a small number of joints in the process, and the B57 antigen indicates multiple lesions.
The pathogenesis of the disease is associated with the production of antibodies to antigens. Antigen-antibody complexes are deposited in the synovium, causing an inflammatory process that is maintained for a long time by a cytokine storm. Long-term psoriatic arthritis destroys cartilage tissue, causes thinning of bone tissue (osteoporosis) and its proliferation with the development of joint deformation, immobility (ankylosis) and loss of function.
Clinical forms of psoriatic arthritis
The following types of PsA are distinguished:
- Distal. The end joints of the fingers are involved in the pathological process. Occurs in 5% of cases.
- Asymmetrical damage to one or more (no more than four) large joints, as well as proximal (located closer to the limb) joints of the fingers. Occurs in two thirds of patients.
- Symmetrical lesions (rheumatoid-like form) occur in a fifth of patients.
- Osteolytic. It manifests itself as dissolution (lysis) of bone joint tissue with a decrease in length and subluxation of the fingers. Osteolysis is possible in all forms of psoriatic arthritis.
- Spondyloarthritic. The sacroiliac joints and spinal joints are affected. Occurs in half of the cases. The combination with psoriatic arthritis of the joints of the extremities develops much less frequently.
Any form of arthritis has serious complications, so you should not delay treatment.
See how easily the disease can be cured in 10-12 sessions.
Herbal preparations
There are other herbal remedies that are effective in treating psoriatic arthritis.
Burdock root tincture is suitable for external and internal use. The peeled and crushed root should be placed in a glass container and filled with alcohol 3 cm above the raw material.
Place in a dark place and leave for 21 days, shaking occasionally. Use the prepared tincture to lubricate affected joints, and also take 1 tablespoon before meals. three times a day.
Aloe compress has an anti-inflammatory and healing effect. The leaves need to be grated and mixed with five drops of vegetable oil. Apply to affected areas in the evening, before bed.
Symptoms of psoriatic arthritis
Signs of psoriatic arthritis depend on the nature of its course.
First signs
Psoriatic arthritis begins on average 6 years after the appearance of changes on the skin. But in recent years, PsA has increasingly preceded skin rashes.
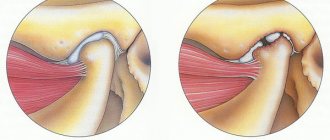
The disease usually begins with the onset of fever, malaise, redness and swelling of the distal interphalangeal joints of the fingers and toes with the development of radish-shaped deformities of the fingertips. Damage to several interphalangeal joints of the finger involving soft tissues is called dactylitis (inflammation of the finger). The finger swells, becomes reddish-bluish in color and looks like a sausage. All this is accompanied by severe pain.
Swelling, redness of the joint and fever are the first signs of psoriatic arthritis
Much less often, the first symptoms of psoriatic arthritis appear in one or two large joints. The lesions are asymmetrical, most often the ankles are affected, and then the inflammation rises like a ladder with the knee affected. Characterized by morning stiffness of movement, which goes away after a while. Less commonly, symmetrical damage to large joints occurs, most often the knees - a rheumatoid-like form.
When the first symptoms of psoriatic arthritis appear, you should immediately consult a doctor to stop the progression of the disease as quickly as possible.
Obvious symptoms
Characteristic signs of psoriatic arthritis include:
- distal lesions of the fingers with simultaneous lesions of the nails; development of dactylitis with sausage-shaped fingers;
- asymmetrical damage to 2 – 3 large joints with the formation of mono- and oligoarthritis (damages of one or more joints) and enthesitis (inflammation of the tendon attachment site); pain in psoriatic arthritis intensifies in the morning and decreases after the start of physical activity; The joints of the lower extremities (knees, ankles) are especially often involved in the pathological process; sometimes the inflammation spreads to multiple joints;
- the process also involves the joints of the lumbosacral spine and sacroiliac joints; this is accompanied by pain and movement disorders: the back does not straighten;
- the course of the disease is undulating: exacerbations alternate with partial (less often complete) remissions; often psoriatic arthritis worsens against the background of progression of skin symptoms of psoriasis.
If obvious symptoms of psoriatic arthritis appear, it is not too late to seek medical help: you can help the patient in any case.
Dangerous symptoms, recommendations
You should consult a doctor immediately if:
- many joints become inflamed at once - a sign of generalization of the process;
- pain appears in the lower back - a symptom of psoriatic arthritis of the spinal joints;
- the appearance of joint dislocations and subluxations.
These symptoms of psoriatic arthritis indicate an unfavorable course of the disease and require immediate medical attention.
Psoriatic arthropathy
The uniqueness of psoriatic arthritis (PA) consists of combined damage to the joints of the extremities and spine, a wide variety of clinical symptoms, variability of initial manifestations, serological and radiological negativity in the early stages. Being one of the forms of disease of the joints and spine, PA, along with ankylosing spondylitis, Reiter’s disease and other reactive arthritis, belongs to the group of seronegative arthritis [2, 17].
The disease generally begins between the ages of 20 and 50, although cases of PA in children are not uncommon. Badokin V.V. (2005) indicates that predictors of an unfavorable course of PA are young age and male gender.
The reasons for the development of PA remain unclear; genetic, immunological and environmental factors can be identified among the formation factors. However, the basis of the pathogenetic mechanism is the activation of cellular immunity in individuals with a congenital predisposition. The participation of immunological factors in the pathogenesis of PA is confirmed by the detection of cellular infiltrates both in the skin and in the tissue of the affected joints, the deposition of immunoglobulins in the epidermis and synovial membrane. In the serum, an increase in immunoglobulins class A (Ig A) (in 90%) and G (IgG), circulating immune complexes (CIC) is primarily determined; antibodies to skin components and antinuclear antibodies are detected [2, 12, 18]. There are quite clear signs of a violation of not only humoral, but also cellular immunity (decreased T-lymphocyte response, decreased suppressor cellular function). It has now been proven that the key point in the inflammatory response in psoriasis is the expression of tumor necrosis factor-a (TNF-α) [2, 12, 17].
It is impossible not to take into account the influence of factors such as bacterial, viral and other types of infection (chlamydial, etc.). The possible role of infection, including viral infection, in the etiology of PA is discussed as pathogenetic factors [12, 14, 20]. An exacerbation or even the onset of PA after a joint injury is often observed [12, 14, 15].
Disorders of calcium metabolism play an important role in the pathogenesis of PA [8]. One of the reasons for impaired calcium metabolism is a decrease in its absorption in the small intestine, which is facilitated by impaired fat absorption and changes in protein metabolism. The changes in calcium metabolism identified in patients with PA are directly related to the severity of the pathological process. Since calcium ions act as mediators of cellular receptors through which nervous and humoral reactions are carried out, hypocalcemia and calcium redistribution disorganize this regulation, therefore, a violation of numerous functions mediated by calcium occurs. At the same time, not only disturbances of calcium metabolism, but also changes in the calcium-regulating hormonal system play a role in the pathogenesis of PA. In this case, a balanced hormonal restructuring of parathyroid hormone and calcitonin occurs. The general direction gives grounds to consider these changes as the result of a “protective” metabolic adaptation, ensuring the maintenance of the stability of calcium metabolism in the conditions of the dermato-articular process [8, 19].
The severity of morphological changes in PA depends on the localization of the articular process and the duration of the disease. It has been proven that the more pronounced the synovitis in PA, the more morphologically it differs from rheumatoid arthritis. The outcome of the disease can be fibrous and bone ankylosis. Continued proliferation leads to bone destruction, ultimately causing the formation of newly formed bone and subsequently perverse joint remodeling [3, 5, 7, 9, 10, 11, 12, 20].
When diagnosing PsA, dermatologists most often focus on one single sign - the presence of psoriatic rashes in combination with arthritis. However, PA has its own characteristic symptom complex:
- the presence of psoriatic plaques, dystrophic changes in nails;
- parallelism of the course of skin and joint syndromes;
- arthritis of the distal interphalangeal joints of the hands (at the onset of PA, larger joints are rarely affected);
- damage to the metacarpophalangeal, proximal and distal interphalangeal joints (axial damage);
- paraarticular phenomena (sausage-shaped defiguration of fingers);
- seronegativity for rheumatoid factor;
- characteristic x-ray picture [3, 5, 6, 8, 10, 11, 19].
The asymmetry of radiological symptoms and pronounced phenomena of secondary osteoarthritis are important; cyst-like clearings in combination with sclerotic changes, focal compaction of the bone structure, and marginal outgrowths. The asymmetry of joint damage characteristic of PA can be expressed not only in the right or left side of the lesion, but also in the degree of joint damage.
The severity of PA almost always correlates with the severity of the skin process. Thus, focal vulgar psoriasis is usually associated with the development of distal or mono-oligoarthritic variants of the articular syndrome and long-term preservation of the functional ability of the musculoskeletal system. At the same time, exudative and especially atypical dermatosis is most often accompanied by the development of generalized arthritis, osteolytic and spondyloarthritic variants, a rapidly progressive course. As for the malignant form of Psoriasis, which occurs as pseudosepsis with clear general and visceral pathology, it is extremely rare in cases of severe forms of psoriasis with a constantly relapsing course.
Exacerbations of PA may be accompanied by changes in laboratory parameters - ESR accelerates (up to 60 mm/hour or more), anemia develops (Hb up to 50 g/l and below), resistant to therapy. Severe dysproteinemia with a decrease in albumin and hypergammaglobulinemia (up to 35% or more) is possible.
An exacerbation of the disease is almost always accompanied by an increase in body temperature to febrile. Along with the subsidence of the activity of the process and the resolution of exudative phenomena in the joints, the temperature also normalizes. Sometimes, with malignant forms of PA, the fever is intermittent, accompanied by chills and heavy sweat, reminiscent of the picture of sepsis.
The problem of differential diagnosis of PA has not lost its relevance at present. This is explained by the fact that PA is an extremely diverse disease in its clinical manifestations and does not always fit into the developed criteria. Be sure to pay attention to signs that are not characteristic of PA:
- No psoriatic rashes.
- Seropositivity for rheumatoid factor.
- Rheumatoid nodules.
- Tophi.
- There is a close connection between articular syndrome and urogenital and intestinal infections [3, 5, 6, 8, 9, 12, 14].
Sometimes dermatologists overlook spinal lesions in PsA. In more than 50% of patients with psoriasis, spondyloarthritis is not diagnosed. Although the presence of spondyloarthritis and certain sacroiliitis is a differential sign of PA. This is of particular importance in women aged 20–30 years with symmetrical damage to the proximal joints of the hands and feet, when the differential diagnosis of PA and rheumatoid arthritis (RA) becomes more complicated. An additional diagnostic sign of RA is a positive Valera-Rose reaction. It is known from history that at first spondyloarthritis in psoriasis was diagnosed as an atypical variant of RA. The discovery of rheumatoid factor made it possible to identify PA as an independent disease, and to classify spondyloarthritis in psoriasis as a secondary lesion of the joints.
Secondary spondyloarthritis also includes Reiter's syndrome, Behçet's syndrome, arthritis in ulcerative colitis and Crohn's disease. Some characteristic common features were noted for all diseases of this group: infectious trigger factor, family history, genetic predisposition. Often in one patient one can find clinical manifestations of PA and Reiter's disease, Reiter's disease and inflammatory bowel disease (Crohn's disease, Whipple's disease), acute intestinal infections and manifestations of Reiter's disease.
In recent years, the number of patients with Reiter's disease (RD), a multisystem disease with a complex pathogenesis, in which autoimmune mechanisms play an important role, and the trigger agent of the disease is chlamydia, has been increasing. It must be remembered that if the triggering agent of the disease is enterobacteria (Salmonella, Shigella, Yersinia), then with a similar clinical picture of joint damage, one speaks not of BD, but of Reiter's syndrome. As a rule, BD develops in individuals with a genetic predisposition to joint disease, especially the intervertebral and sacroiliac joints. The HLA-B-27 system antigen is detected in the phenotype of patients in 80% of cases. In BD, there is a connection between the disease and gender, with the ratio of men to women usually considered to be 20:1. The main signs of the disease (urethroprostatitis, arthritis, conjunctivitis, and, less commonly, lesions of the skin, mucous membranes and internal organs) occur in patients in different sequences and are characterized by varying degrees of severity of the clinical course. The difficulty of diagnosis usually arises with “incomplete” forms or in cases where the patient has all the main signs of BD, but they occur after long periods of time, appear unnoticeably, or at certain stages of the disease one or two symptoms dominate. In BD, unlike psoriatic arthritis, chlamydial urethritis, as a rule, precedes joint damage; anti-chlamydial antibodies are often found in the blood of patients. PA is characterized by asymmetry of joint damage, which can be expressed not only in the right or left side of the lesion, but also in the degree of joint damage. Articular lesions are usually benign; there is pain when loading the affected joint; joint lesions usually begin in the lower extremities (“staircase symptom”), arthritis appears “spiral-shaped,” i.e., the inflammatory process begins more often in large joints; muscle atrophy is typical, noted already at the onset of the disease. Important differential signs are the lack of synchrony in the occurrence of articular and skin symptoms, balanitis, as well as ring-shaped erosions with areas of desquamation of the whitish mucous membrane on the tongue, oral mucosa and upper esophagus [8].
Ankylosing spondylitis (ankylosing spondylitis) is characterized by:
- pain in the lumbar and sacral region;
- persistence of pain syndrome;
- night pain at rest, especially in the second half of the night and in the morning, often combined with stiffness and tension in the rectus back muscles;
- reduction of pain after exercise;
- lumbodynia, ischalgia;
- chest pain that gets worse with coughing and sneezing;
- disturbance of general health (fatigue, weight loss, low-grade fever, sweating);
An objective examination reveals the clinical syndrome of sacroiliitis and unstable arthritis, especially of the joints of the lower extremities; the presence of proteins of the acute phase of inflammation (increased ALT, AST, total protein, seromucoid, increased thymol test, etc.); presence of HLA-B-27 antigen; X-ray signs of damage to the sacroiliac joints (bilateral sacroiliitis) [8, 19].
In elderly people with a combination of joint damage and psoriasis, it is necessary to carry out a differential diagnosis with osteoarthritis. Osteoarthritis is a widespread degenerative, often age-related, damage to articular cartilage and adjacent bone tissue. It occurs more often in people over 40 years of age. Most patients with osteoarthritis suffer from deep, dull pain that is aggravated by physical activity and relieved by rest. In severe cases, pain may continue even during sleep, which may be a false sign of PA. Morning stiffness, unlike other inflammatory joint diseases, with osteoarthritis is short-lived and lasts no more than 20 minutes. The “gel phenomenon” is characteristic - the occurrence of swelling of the joint after prolonged immobilization. The main differential sign should be characteristic radiographic changes in osteoarthritis [1, 14, 18].
Treatment
Treatment of PA should be aimed at solving the following objectives: reducing pain and inflammation, reducing the frequency of exacerbations and damage to new joints, improving quality of life, slowing the progression of the pathological process and preventing disability. Thus, based on the pathomorphological changes in the joints during PA and our own experience, the treatment of PA should be long-term, complex, including, along with anti-inflammatory therapy, vascular agents that improve microcirculation, muscle relaxants, chondroprotectors; agents for the treatment of osteoporosis; physiotherapeutic methods and rehabilitation measures.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are among the most important “symptomatic” medications. This is determined by a unique combination of anti-inflammatory, analgesic, antipyretic and antithrombotic properties, covering almost the entire spectrum of the main symptoms most characteristic of diseases of a rheumatic nature. Such a simultaneous combination of positive effects is not observed in any of the drugs known in medicine.
NSAIDs are similar in pharmacological properties, biological activity and mechanisms of action, which are primarily associated with blockade of the synthesis of cyclooxygenase, a key bifunctional enzyme involved in the regulation of prostaglandin synthesis. Thus, they have a double effect - they eliminate pain and weaken the inflammatory process. Without them, it is difficult to imagine treating PA.
Currently, the class of “traditional” NSAIDs includes about 20 drugs, which according to their chemical structure are divided into several groups: derivatives of salicylic, indole, heteroarylacetic, propionic and enolic acids, etc. All “traditional” NSAIDs have a number of common chemical and pharmacological properties . Being weak organic acids, they are well absorbed in the gastrointestinal tract (GIT), bind to albumin and have approximately the same volume of distribution [4]. It is necessary to remember the “golden” rule - individual selection of NSAIDs for each patient. In reality, the choice of NSAID is usually empirical and largely based on the physician's personal experience. There is a point of view on the advisability of using the least toxic drugs at the beginning of treatment, which include propionic acid derivatives (ibuprofen, flurbiprofen, ketoprofen, naproxen, etc.). The dose of NSAIDs should be gradually titrated to an effective dose, but not exceeding the maximum allowable, over 1-2 weeks and, if there is no effect, try using a different drug or drugs. Prescribing simple analgesics can reduce the need for NSAIDs. It should be borne in mind that an important characteristic of this group of drugs is the “half-life” of the active substance. Depending on the “half-life” limits, NSAIDs are divided into 2 main categories: short-lived (half-life less than 6 hours) and long-lived (half-life more than 6 hours). However, synovial concentrations of drugs may exceed serum concentrations and the clearance time of short-lived drugs may be prolonged. For example, prescribing ibuprofen 2 times a day is as effective as taking the drug 4 times a day. It is also necessary to synchronize NSAIDs with the rhythm of clinical activity, which can increase the effectiveness of treatment [8]. But, unfortunately, all NSAIDs have their own “Achilles heel” - they cause many side effects from the digestive system, kidneys and liver. The risk of such complications especially increases with long-term use. Side effects of NSAIDs are divided into:
- Subjective: nausea, vomiting, dyspepsia, diarrhea, constipation, heartburn, pain in the epigastric region.
- Objective: erosions and ulcers detected by endoscopic (or x-ray) examination.
- Severe complications: perforated ulcers, bleeding.
Subjective side effects are observed in a third of patients, more often with long-term use of NSAIDs, and in many cases are the reason for interruption of treatment during the first months of therapy. However, their development does not correlate well with the true severity of gastrointestinal damage. Being weak organic acids, they are well absorbed in the gastrointestinal tract, bind strongly to albumin and have approximately the same volume of distribution. Hypoalbuminemia leads to an increase in the serum concentration of the drug, which causes increased toxicity. The risk of such complications especially increases with long-term use. That is why, in recent years, special attention has been drawn to elderly and senile patients who suffer from a variety of concomitant diseases and take medications that increase the risk of side effects of NSAIDs. Such drugs include direct and indirect anticoagulants, low doses of acetylsalicylic acid, glucocorticoids, methotrexate, cyclosporine and many others. In addition, NSAIDs are prescribed to many patients suffering from hypertension and heart failure. At the same time, NSAIDs reduce the effectiveness of b-blockers, angiotensin-converting enzyme (ACE) inhibitors and diuretics.
Among the “standard” NSAIDs, piroxicam and indomethacin have the greatest ulcerogenic activity, and ibuprofen (in low analgesic doses) and especially selective cyclooxygenase-2 (COX-2) inhibitors have the least. It is possible to reduce side effects by prescribing NSAIDs in suppositories. In the distal segment of the digestive tract, due to anatomical and physiological features (rich venous network), there is a high percentage of drug absorption and the absence or extremely insignificant participation of digestive enzymes. As a rule, the intake of substances adsorbed in the rectum occurs simultaneously through the circulatory and lymphatic systems, which have a special development in this area. Thanks to the first system, the active substances are quickly delivered to the systemic circulation, and the second ensures their prolonged action. In this case, only a very small part of the adsorbed drugs enters the portal vein, which carries blood from the internal organs to the liver.
It is desirable that the basic drug in the treatment of PA, which is NSAIDs, meet several criteria: the drug should provide clinical and laboratory improvement, which should last for some time after its discontinuation, should inhibit bone and cartilage destruction and have fewer side effects. Therefore, at the present stage in medicine, a new series of drugs has appeared: nimesulide, celecoxib, lornoxicam, meloxicam, infliximab.
Nimesulide entered clinical practice several years ago simultaneously in several countries and continues to be registered in others. Nimesulide was the first marketed drug with a preferential inhibitory effect on cyclooxygenase type 2 (COX-2) compared to COX-1, the selectivity of which was first shown in 1995 by several research groups and reconfirmed this effect at a later time. Currently, under various trade names, it is registered and sold in 50 countries in various release forms. The undoubted success of the drug is associated not only with its anti-inflammatory, analgesic and antipyretic effects, but also with some unique pharmacological and clinical properties. Nimesulide is characterized by a relatively rapid onset of analgesic effect, low toxicity to the gastrointestinal tract and kidneys, and good tolerability when used by patients with respiratory problems caused by taking other NSAIDs. The main pharmacological and pathophysiological properties of nimesulide are associated with the selectivity of action on COX-2, as well as with a decrease in the release and decrease in the biological effect of inflammatory mediators (cytokines, histamine, enzymes that degrade the structure of cartilage, superoxide anion radical) produced by various cells.
Nimesulide, celecoxib, meloxicam are direct descendants of NSAIDs, but only along one line: they act specifically on COX-2, but do not affect COX-1. COX-1 is a constitutional enzyme, i.e., constantly functioning normally in the body, mainly affecting the production of prostaglandins, which protect and regulate normal cellular processes in the gastrointestinal tract and platelets. As a result, while maintaining their therapeutic effect, these drugs do not have harmful effects on many organs, including the stomach. These drugs reduce the risk and frequency of severe stomach damage - gastritis, ulcers and bleeding. The use of these drugs in elderly and senile patients is especially important.
Infliximab belongs to a fundamentally new group of so-called biologically active immunomodulator drugs. The mechanism of their action is associated with the antagonism of one of the central mediators of inflammation - TNF-a. The drug is a chimeric mouse-human IgG1 monoclonal antibody consisting of high-affinity neutralizing mouse monoclonal antibodies to TNF-a and a fragment of the human IgGlk molecule. Forms a stable complex with both soluble and membrane-associated forms of human TNF-a, reducing its functional activity. Reduces the concentration (binds and inhibits synthesis) of interleukin-1 (IL-1); interleukin-6, interleukin-8 and other inducers of inflammation and tissue destruction. Infliximab is eliminated from the body within 6 months. The main criteria for choosing infliximab for therapy in a particular patient are: severe psoriasis, resistant to conventional therapy, the area of skin affected is more than 50%, the duration of the disease is at least 6 months, severe oligo- or polyarthritis [13, 19, 20].
It is possible to prescribe a combination drug of diclofenac sodium (50 mg) and misoprostol (200 mcg). At the same time, misoprostol prevents the negative effects of diclofenac on the mucous membrane and the development of NSAID gastropathy.
Chondroprotectors . One of the pathological manifestations of PA is the destruction of articular cartilage. Cartilage, like other tissues, is remodulated during growth and development, in other words, processes of synthesis and degradation occur in it. Let us recall that articular cartilage consists of two main components: intercellular substance (matrix), which makes up 98% of the volume of cartilage tissue, and cells: chondrocytes and chondroblasts (2%). For the integrity of cartilage throughout life, it is necessary that the constant synthesis of glycosaminoglycans, collagens and hyaluronic acid be equal to the amount lost as a result of natural metabolism. IL-1 inhibits matrix catabolism [1]. The constant synthesis of glycosaminoglycans and collagen depends on the presence of such substances, but with very small amounts of IL-1 their activity is inhibited. It is possible to influence cartilage at different stages of its damage: primary prevention, screening of the asymptomatic stage and preventive treatment (for example, for osteoporosis) or treatment of an already developed disease. The effectiveness of a number of chondroprotective drugs has already been proven - these are chondroitin sulfate, glycosamine sulfate, diacerein, sodium hyaluronate (contains high molecular weight hyaluronic acid), hyaluronic acid administered intra-articularly, etc. Please note that these drugs are mainly dietary supplements . A distinctive feature of this group of drugs is the time of onset of effect, usually 2–8 weeks from the start of treatment, and the persistence of the effect for 2–3 months after cessation of therapy [1].
Treatment of osteoporosis. PA is characterized by the presence of metaphyseal osteoporosis. The amount of bone loss increases with age and is more common in females. X-ray methods are the most accessible and widely used in clinical practice when examining bones. However, X-rays can detect the presence of osteopenia only when there is a loss of more than 30% of bone mass, so this method most often detects late signs of osteoporosis. A modern method for measuring bone density, densitometry, is based on measuring the mineral component of bone tissue, calcium. This is the most sensitive method for detecting osteoporosis and assessing its severity. Densitometry is necessary to confirm the diagnosis of osteoporosis, assess the risk of fractures, and monitor the adequacy of treatment. When choosing a treatment method for osteoporosis, there must be firm confidence in its effectiveness in preventing fractures and their consequences. The expected result should significantly outweigh the potential danger of therapy associated with possible side effects.
Physiotherapeutic methods and rehabilitation measures. An important condition for the success of treatment of patients with PA is also physical therapy and comprehensive rehabilitation measures. Widely used physiotherapeutic methods of treating PA reduce pain, muscle spasms, inflammatory processes, improve microcirculation and trophism, and have a beneficial effect on metabolic processes in joint tissues.
They use ultraviolet irradiation, UHF electric field, low-frequency alternating magnetic fields, electrophoresis of Analgin, Novocaine, Trimecaine, Dimexide on the area of the affected joint. During the period of subsiding exacerbation, as well as in the initial stage of the disease, when the symptoms of synovitis are weakly expressed or absent, exposure to electromagnetic fields of high and ultra-high frequencies (inductothermy, decimeter and centimeter wave therapy), pulsed currents of low frequency - sinusoidal modulated and diadynamic, magnetic therapy, laser exposure, hydrocortisone phonophoresis. To stimulate the trophism of articular cartilage, electrophoresis of lithium, calcium, sulfur, zinc, and Humisol is performed.
Of the various physiotherapeutic methods, medicinal electrophoresis, which combines the therapeutic effects of direct electric current and a medication administered with its help, has proven itself well.
For PA with pain syndrome without clinical synovitis, proliferative phenomena, vasotrophic disorders, contractures, thermal procedures are indicated, including applications of paraffin, ozokerite, silt, and peat mud. In the remission stage, sea, radon, sulfide, iodine-bromine, and bischofite baths are effective. We should not forget about the beneficial effect of therapeutic massage on muscle-articular tissue, which reduces muscle spasm, increases the tone of weakened muscles, stimulates trophism of the affected joints and improves the patient’s functional abilities. Massage performed outside of an exacerbation of PA should be gentle on the affected joints; it is necessary to avoid mechanical irritation of the joint capsule; Particular attention should be paid to working with the muscles adjacent to the joint.
For questions regarding literature, please contact the editor.
Yu. A. Gallyamova , Doctor of Medical Sciences, Associate Professor of the Russian Medical Academy of Postgraduate Education , Moscow
Why is PsA dangerous?
Psoriatic arthritis occurs in different ways. But even an imperceptible course can lead over time to permanent loss of ability to work. To find out the degree of danger of the disease, you need to undergo an examination.
Degrees of psoriatic arthritis
During the course of the disease, the following degrees of activity are distinguished:
- Minor.
It manifests itself as slight pain in the affected joints during physical activity. Stiffness in movements in the morning after sleep lasts no more than half an hour or is completely absent. There is no fever, laboratory signs of the inflammatory process are minimal: ESR is not higher than 20 mm/hour. - Average.
During exacerbations, a slight fever appears, the joints may swell slightly, the pain is moderate, and appears at rest and during movement. Stiffness after sleep lasts up to three hours and goes away with physical activity. Laboratory parameters changed significantly: ESR up to 40 mm/hour, increased number of leukocytes. - Expressed.
Severe fever during an exacerbation, joints swell, the skin over them turns red, the pain is very strong and constant. Stiffness after sleep lasts more than three hours. Laboratory indicators indicate the presence of a severe inflammatory reaction.
Chondroprotectors: what are they, how to choose, how effective are they?
Joint pain at rest
Possible complications
Untreated psoriatic arthritis can progress and lead to complete loss of joint function and disability. During an exacerbation, in some cases the following complications occur:
- the occurrence of articular subluxations and dislocations;
- melting (lysis) of the distal ends of the bones of the fingers and toes;
- generalization of the process - a severe progressive course with multiple joint lesions;
- ankylosis - complete loss of joint function, impaired mobility of the limb.
What to do during an exacerbation of psoriatic arthritis
In case of exacerbation, accompanied by high fever, swelling, redness, joint pain, the following recommendations must be followed:
- take orally a tablet of medication from the group of non-steroidal anti-inflammatory drugs (NSAIDs) - Nise, Diclofenac, Meloxicam, Celebrex;
- apply a gel or cream with the same products to sore joints several times a day;
- to reduce swelling, you can take an antihistamine - Claritin, Zodak, etc.;
- call a doctor at home.
If the disease worsens, you can take the anti-inflammatory drugs Nise, Diclofenac, Meloxicam, Celebrex, as well as the antihistamine Claritin or Zodak
Clinical observation
Patient D., 11 years old, came for consultation with complaints of rashes on the skin of the torso, upper and lower extremities without subjective sensations.
History of the development of the present disease.
According to her mother, she has been ill since the age of five, when pain in her right heel first appeared with rapid progression, and therefore she consulted a rheumatologist at her place of residence, where she was diagnosed with juvenile rheumatoid arthritis. In 2012, pain and swelling appeared in the shoulder, elbow, ankle, and wrist joints, but did not receive adequate treatment. In 2013, she was consulted for the first time at the Federal State Budgetary Institution NIIR named after. V.A. Nasonova, where a diagnosis of juvenile rheumatoid arthritis was made and therapy was prescribed with methylprednisolone at a dose of 4 mg/day, which she received until December 2015. The patient also received basic therapy with methotrexate 10–12.5 mg/week, non-steroidal anti-inflammatory drugs almost constantly. During the first two years, the therapy provided a positive effect, but since the dose of glucocorticosteroids (GCS) was reduced, the above-mentioned complaints began to recur with the greatest manifestation by December 2015 (associated with the abolition of GCS). Thus, taking into account the severity of the child’s condition, early onset of the disease, unfavorable prognosis, functional failure, high clinical and laboratory activity, the girl was hospitalized for a full clinical and laboratory examination and to decide on treatment correction. The progressive nature of the disease, refractoriness to the therapy, and the clinical variant of the disease were the rationale for prescribing a genetically engineered biological drug, and the clinical features of the disease made it possible to select the T-lymphocyte costimulation inhibitor abatacept at a dose of 10 mg/kg per infusion as a preferable alternative. In the children's department of the Moscow Center for Dermatovenereology and Cosmetology, abatacept therapy was initiated on May 19, 2016 at a dose of 300 mg per infusion with good tolerability and a positive initial effect. Subsequently, she received therapy regularly until November 2021. The first appearance of rashes on the skin of the hands and feet was noted in November 2021, and therefore methotrexate and abatacept were discontinued; in December, abatacept infusions were resumed after relief of dermatitis. The next hospitalizations were in February 2017 and February 2018. The last hospitalization was in May 2019 at the Federal State Budgetary Institution NIIR named after. V.A. Nasonova, where therapy was carried out with methotrexate 15 mg subcutaneously, abatacept intravenously at a dose of 500 mg with positive dynamics in the form of improved gait, increased range of motion in the joints, reduced exudative changes in the joints, and improved muscle tone. A real exacerbation of the skin pathological process has been observed for 2 months, for arthritis he is taking therapy: abatacept 500 mg per infusion once a month, methotrexate 15 mg/week. IM 1 rub./week. Due to the prevalence of the skin process, I contacted the Moscow Center for Dermatovenereology and Cosmetology, Kolomensky branch.
Patient's life story.
A girl from the 1st physiological pregnancy, which proceeded satisfactorily, 1st term spontaneous birth. Psychomotor development by age. Living conditions are satisfactory. Meals are regular.
Past diseases: rare acute respiratory viral infections. Childhood infections: chickenpox in 2012. There were no injuries or operations. Concomitant diseases: juvenile rheumatoid arthritis.
Preventive vaccinations before the disease were carried out according to the age calendar, no reaction to them was noted. Mantoux test 10/23/2018: negative.
Allergological and epidemiological anamnesis are not burdened. Denies tuberculosis, syphilis, malignant tumors, and mental illness. Heredity: not burdened.
Objective examination data:
general condition is satisfactory. Consciousness is clear. The patient's position at the time of examination is active. The physique is normosthenic. Height 164 cm, weight 52 kg, body temperature 36.6 °C, pulse 75 beats/min, rhythmic, blood pressure 110/85 mm Hg. Art. Examination of organs and systems: no features.
Laboratory and instrumental examinations
Increased level of platelets in the blood (440×109/l with a norm of 150–390×109/l), monocytes (0.75×109/l with a norm of 0.09–0.6×109/l), alkaline phosphatase (306 U/L at a rate of up to 300 U/L), rheumatoid factor (849 IU/ml at a rate of 0–15 IU/ml), antibodies to cyclic citrullated peptide (>300 U/ml at a rate of 0–5 U/L) from 05/27/2019.
ECG dated May 27, 2019: change of pacemaker from lower atrial to sinus. Heart rate 51–66 beats/min. Normal position of the electrical axis of the heart. Syndrome of early ventricular repolarization. Disruption of ventricular repolarization processes. Disruption of myocardial repolarization processes in the inferior wall of the left ventricle. In lead V1, the QRS complex appears as QS. In a standing position, the rhythm is sinus.
X-ray of the hands and distal feet
dated 05/27/2019: soft tissues are not changed. Periarticular osteoporosis. A few cysts and single erosions in the wrists. The gaps in the individual joints of the wrists are narrowed. Deformation of individual bones of the wrists. Conclusion: X-ray picture of chronic erosive arthritis with a predominance of changes in the bones of the wrists.
X-ray of the cervical spine
dated 05/27/2019: soft tissues are not changed. Physiological lordosis has been straightened. The intervertebral disc spaces are not narrowed. The supporting platforms of the vertebral bodies are smooth. The structure of the bone tissue is not changed. Conclusion: there are no structural changes in the cervical spine.
Status localis.
The pathological skin process is acutely inflammatory and widespread. It is localized on the skin of the anterior abdominal wall, the extensor surface of the elbows, the anterior surface of the thighs, and the extensor surface of the knees. It is represented by pink papules, up to 0.1 cm in size, merging into infiltrated pink plaques, round in shape, with clear boundaries, with silvery peeling on the surface. The psoriatic triad is positive. Dermographism red. Visible mucous membranes are pink and clean. The nail plates of the hands have pinpoint impressions of the “thimble” type; the nail plates of the feet are not changed. Defiguration of the wrist, small joints of the hands, knees, ankle joints, small joints of the feet.
Consultation with Professor E.A. Batkaev
. from 07/31/2019. Diagnosis: “Psoriasis, common form. Psoriatic arthritis." Recommended: domestically produced natural enterosorbent 0.25 g orally 2 times per day 30 minutes before meals for 10 days, cetirizine 15 drops 1 time per day for 10 days, externally lotion with betamethasone + salicylic acid 2 times per day for 10 days. As a result of the therapy, the rash resolved to spots of post-inflammatory hyperpigmentation; the patient is now under observation by a rheumatologist.
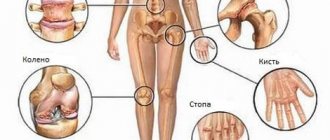
Possible localizations of the inflammatory process
Psoriatic arthritis can affect different joints:
- Arthritis of the lower extremities
– the most common localization. Joints affected:- hip – rare localization, manifested by pain and stiffness of movement; swelling and redness are not typical;
- knee - of the large articular joints, it is most often affected; lesions are often asymmetrical and appear either immediately in one knee, or develop after primary psoriatic arthritis of the joints of the foot (staircase sign);
- ankle - very often the lesion begins with it; severe inflammation and swelling is accompanied by severe pain and impaired movement;
- heel - in the heel area with ankle arthritis, enthesitis develops - inflammation at the internal site of attachment to the heel bone of the Achilles tendon and plantar aponeurosis; there is a slight swelling and severe pain in the heel area;
- interphalangeal joints – several on one or more fingers may be affected primarily; dactylitis develops - inflammation of the finger, and it takes on the appearance of a sausage; Damage to the terminal sections of the fingers and nails is also typical.
- Arthritis of the upper extremities
- also occurs frequently. Joints affected:- shoulder – common location; sometimes this is the only joint affected; swelling, redness, soreness and morning stiffness depend on the degree of activity of the pathological process;
- ulnar - most often affected after the small joints of the hand (staircase symptom); enthesitis often develops in the elbow area, increasing pain;
- small joints of the hand and fingers - psoriatic arthritis of the finger joints affects several of them on one finger at once, and they take on the appearance of sausages; the distal ends of the fingers and nail plates are also affected;
- Lumbosacral arthritis
– affects the joints of the lumbosacral spine. Pain appears in the lower back and buttocks, the function of the spine is disrupted - flexion and extension are first impossible due to pain, and then due to the development of ankylosis. - Sacroiliac arthritis
- develops quite often, is asymmetrical in nature, manifested by pain in one side of the back, radiating to the groin area.
Read all about arthritis and its symptoms here.
Reviews on the effectiveness of alternative methods of therapy
Irina: “My grandmother suffered from mild psoriatic arthritis.
Therefore, there was no need to use potent medications. Instead, she willingly used herbal tinctures for rubbing - prepared from birch buds and burdock root.” Anastasia: “Last year I was diagnosed with psoriatic arthritis, which affects my fingers. In two months I dealt with it thanks to comprehensive treatment. “I went to physical therapy at the medical center, and at home I additionally used my own ointment made from hops, chamomile and eucalyptus oil.”
Traditional medicines - infusions, ointments and compresses - can significantly reduce the manifestations of psoriatic arthritis. However, for absolute recovery, a comprehensive, multi-faceted approach is required, which includes following a special diet, using external remedies, taking medications, performing therapeutic exercises and maintaining a healthy lifestyle.
How to establish the correct diagnosis?
Ultrasound and x-rays are often used to diagnose psoriatic arthritis.
Diagnosis of psoriatic arthritis is carried out according to anamnesis (patient survey) and characteristic signs of the disease. The diagnosis is confirmed by laboratory and instrumental studies:
- Laboratory.
Blood tests are carried out - general clinical, biochemical, genetic - to identify signs of the inflammatory process, the presence or absence of rheumatoid factor (to exclude rheumatoid arthritis), antigens that support the inflammatory process. - Instrumental diagnostics:
- radiography of the hands, feet, pelvis, lumbosacral spine and all other interested joints;
- Ultrasound – determination of the volume of joint fluid and enthesitis;
- MRI – for early detection of articular changes in the spine and sacroiliac joints.
Treatment of psoriatic arthritis
After the final diagnosis is established, psoriatic arthritis is treated. It must be comprehensive and selected individually for each patient. Goal of treatment:
- suppression of inflammation activity and disease progression;
- prevention of destruction of articular joints and loss of their function.
It is impossible to completely cure psoriatic arthritis. But modern medicine has the ability to control and manage this disease, provided that treatment is carried out as prescribed and under the supervision of the attending physician. A significant increase in the duration of remission is quite possible.
Drug and non-drug methods are used to treat psoriatic arthritis. If necessary, use folk remedies and surgical methods.
Crunching in joints - when to worry
Intra-articular injections of hyaluronic acid
Drug therapy
Complex drug therapy for psoriatic arthritis includes the following medications:
- Medicines from the NSAID group are prescribed during an exacerbation to suppress inflammation, swelling, pain, and also as an antipyretic. Diclofencac, Ibuprfen, Nimesulide and other drugs are prescribed in the form of tablets for oral administration, intramuscular injections, ointments and gels for external use.
- Glucocorticoid hormones are used for severe inflammation, swelling and pain that is not relieved by NSAIDs. Hormones (Prednisolone, Dexamethasone, Betamethasone, etc.) are taken orally, administered in the form of intramuscular and intra-articular injections.
- Basic drugs that suppress the activity of the immune system (immunosuppressants) - Methotrexate, Cyclosporine, Sulfasalazine, Leflunomide are prescribed in long courses under laboratory and radiological control.
- Genetically engineered biological drugs that contain antibodies, cytokines and other biologically active substances that take part in immune reactions and suppress the activity of pro-inflammatory cytokines - Rituximab, Ustekinumab. Effective modern therapy for PsA.
Correctly prescribed drug therapy allows you to completely control the course of the disease.
Non-drug treatments
Treatment of psoriatic arthritis should be comprehensive and necessarily include therapeutic exercises, reflexology and physiotherapeutic procedures
Complex therapy also includes treatment of psoriatic arthritis using non-drug methods:
- Mode.
During an exacerbation - the most gentle regimen, with a severe exacerbation - bed rest. During remission, a gradual increase in physical activity is recommended. - Nutrition.
There is no special diet, but it is recommended to adhere to the principles of a healthy diet with the exception of fatty, fried, spicy, smoked foods, sweets, baked goods and alcohol. - Physiotherapeutic procedures.
The procedures that are most suitable for the patient’s condition are selected: those that relieve inflammation and pain, restore joint function, eliminate the effects of stress, etc. - Physiotherapy.
Specially selected exercises relieve morning stiffness and reduce pain. During remission, it is recommended to gradually increase the load. - Reflexology.
Acupuncture sessions and other oriental techniques eliminate pain, inflammation, and restore joint function.
Diagnosis and treatment
PsA is diagnosed based on the CASPAR criteria, which were developed by W. Taylor et al. in 2006 [5]. These criteria showed high sensitivity and specificity (0.987 and 0.914, respectively) at early and late stages. According to them, patients must have signs of inflammatory joint disease, which include arthritis, enthesitis, spondylitis, as well as 3 or more points from the five categories presented in Table 1.
Psoriasis and PsA belong to the group of T-cell-mediated diseases, the pathogenesis of which is based on the activation of cellular immunity in the skin and synovial fluid with overproduction and imbalance of key cytokines (pro-inflammatory and anti-inflammatory), which include tumor necrosis factor alpha, interleukins 1, 1b, 6 , 12, 17, 23 and chemokines [6], in this regard, patients with severe forms of psoriasis, especially PsA, require long-term systemic anti-inflammatory and targeted therapy, including the use of basic anti-inflammatory and modern genetically engineered biological drugs.
Therefore, correct and timely diagnosis of joint damage and comorbid pathology is extremely important. Below is a description of clinical observation in the clinical diagnostic department of the Moscow Center for Dermatovenereology and Cosmetology, Kolomensky branch in 2019.
General clinical recommendations
All patients suffering from PsA are recommended to:
- during an exacerbation, strictly follow all doctor’s instructions and do not self-medicate;
- during remission, conduct courses of anti-relapse treatment; regularly perform complexes of therapeutic exercises; It is useful to carry out sanatorium-resort treatment once a year in the sanatoriums of Zheleznovodsk, Pyatigorsk, Kislovodsk, Matsesta, etc.;
- promptly treat all existing concomitant diseases and foci of infection, avoid stress and heavy physical activity;
- eat properly and in a timely manner, lose excess weight;
- get rid of bad habits: smoking and alcohol abuse.
We combine proven techniques of the East and innovative methods of Western medicine.
Read more about our unique method of treating arthritis
Frequently asked questions about the disease
Is it possible to get disability?
If there is a dysfunction of the joint, then yes, it is possible.
Which doctor treats you?
Two doctors treat: a dermatovenerologist and a rheumatologist, but the main one is a rheumatologist.
What prognosis do doctors usually give?
It all depends on the clinical form of the disease and the rate of its progression. But in any case, the disease can be brought under control.
Psoriatic arthritis is not a death sentence; it can and should be treated at any stage of the disease. It is quite possible to relieve the patient from exacerbations, joint pain and progressive decline in function for a long time (sometimes until the end of life). Doctors at the Paramita clinic have extensive experience in treating this disease, please contact us!
Literature:
- Kungurov N.V. et al. Genetic factors in the etiology and pathogenesis of psoriasis // Bulletin of Dermatology and Venereology. 2011. No. 1. pp. 23–27.
- Yusupova L. A., Filatova M. A. Current state of the problem of psoriatic arthritis // Practical Medicine. 2013. No. 3. pp. 24–28.
- Korotaeva T.V. Standards for the treatment of psoriatic arthritis // Scientific and practical rheumatology. 2009. No. 3. P. 29–38.
- Haroon M., Gallagher P., FitzGerald O. Diagnostic delay of more than 6 months contributes to poor radiographic and functional outcome in psoriatic arthritis. Ann Rheum Dis. 2015;74(6):1045–1050. DOI: 10.1136/annrheumdis-2013-204858.
Themes
Arthritis, Joints, Pain, Treatment without surgery Date of publication: 04.11.2020 Date of update: 14.12.2020
Reader rating
Rating: 5 / 5 (1)
Recipes for effective traditional medicines
In home therapy for psoriatic arthritis, widely known, reliable and effective folk remedies such as celery root, birch and lilac buds, marsh cinquefoil and wood lice are mainly used.
Lilac bud tincture
Lilac bud tincture has strong analgesic and anti-inflammatory properties.
To prepare it, you should collect raw materials in an ecologically clean area in early spring.
Two glasses of lilac buds must be filled with medical alcohol or high-quality vodka in an amount of 500 ml.
Leave in a dark place for two weeks and shake vigorously from time to time. Strain the finished product thoroughly and use it to rub the affected areas.
Celery root infusion
Celery root rightly plays one of the leading roles in the folk treatment of psoriatic arthritis. To prepare an effective healing infusion, you need to pour one tablespoon of thoroughly washed and chopped celery into two glasses of boiling water and place it in a dry, dark place. The product should infuse for 4 hours. After this, it should be strained through a strainer or gauze and poured into a dark glass container. Take 2 tbsp. infusion before meals, twice a day for two weeks. For taste and to enhance the beneficial effect, you can add a little honey.
Birch bud decoction
Birch buds are rich in ascorbic acid, fatty acids, grape sugar, tannins, phytoncides and other components that ensure rapid healing of the skin.
Two tablespoons of kidneys should be poured into two glasses of boiling water and left for one hour.
It is very convenient to use a thermos for these purposes. The finished decoction must be drunk within one day, divided into four equal parts.
Marsh cinquefoil ointment
Marsh cinquefoil is another well-known plant that is used for joint diseases due to its warming, analgesic and wound-healing effect.
An ointment for the treatment of psoriatic arthritis can be easily prepared on its basis.
To do this you will need:
- 1 tube or jar of any hypoallergenic cream, maybe for children;
- 3 drops of vitamin E;
- 1 tsp honey;
- 1 tsp alcohol solution of red pepper.
Mix the ingredients thoroughly until smooth and apply to affected areas of the body 2 times a day. This product must be stored in the refrigerator.
Chickweed herb compress
Woodlice grass is a unique herbal remedy rich in vitamins C, E and K, as well as zinc, magnesium, iron, organic acids, essential oils, lipids and tannins. For psoriatic arthritis, compresses are made from this plant that can relieve pain and heal lesions.
Fresh herbs must be steamed and wrapped in gauze, and then the resulting compress must be applied to the affected area of the body for 20-30 minutes.
Wraps
For wraps for psoriatic arthritis, it is recommended to use fresh whole leaves of cabbage and coltsfoot.
They are applied to a clean skin surface, after steaming and smearing with a small amount of honey.
Lilac leaf wraps are also effective.
In a steamed state, they need to be applied to the sore joints, secured with a bandage and insulated with a towel. The therapeutic effect will occur in two weeks.
Therapeutic baths
A significant therapeutic effect is provided by baths based on coniferous plants. To do this, you need to pour a few spruce or pine branches into a pan of boiling water, leave for 15-20 minutes and pour into a bath of warm water. It is recommended to do the procedure no longer than half an hour. For maximum therapeutic effect, 7-8 baths are required, with a three-day break between them.
Similar baths can be done with string and chamomile.