What is osteoporosis of the knee joint
With osteoporosis of the knee joint, the symptoms are not obvious at the initial stages, but timely treatment helps to avoid further development of the pathology. The disease manifests itself in deformation of tissues and joints. The disease can affect both the skeletal system in general and individual parts. The knee joints cease to be elastic, which leads to severe spasms when walking. Failure to detect the disease in a timely manner can result in irreversible consequences. Bone deformities can make a person disabled.
Fractures happen unexpectedly, osteoporosis creeps up unnoticed
Having talked about the causes of osteoporosis, it is necessary to understand the forms of its manifestation. The main mistake of many doctors lies in the fact that they often mistake symptoms of other diseases for manifestations of osteoporosis. In reality, osteoporosis manifests itself with minor symptoms with an almost complete absence of complaints; very often the disease is detected only in the presence of fractures. This feature of the disease has given scientists reason to call osteoporosis a “silent epidemic.” Of course, with osteoporosis, there are back pains, but these are aching pains of “fatigue” that arise only after a relatively long (more than 30 minutes) stay in one static position - standing or sitting. Other indirect signs of the disease include senile stoop (hunchback), night leg cramps, increased fatigue, periodontal disease, brittle nails and premature graying. And although the presence of these symptoms is not a 100% confirmation of the diagnosis, it still allows us to determine the range of studies necessary to clarify it.
Causes of the disease and risk factors
Various factors can cause osteoporosis of the knee joint. Most often, the appearance of the disease is associated with low calcium levels in the body. Calcium promotes the formation of oxyapathates, which are involved in the formation of bone tissue. When calcium levels fall, the risk of developing osteoporosis increases. Lack of zinc, phosphorus, vitamins D and B leads to the development of the disease. The reason for the lack of these elements may be a violation of absorption by the body. Chronic diseases, alcohol abuse, excess weight, and some medications lead to pain in the knee area.
Diagnostics
If signs of the disease appear, you should consult a general practitioner, rheumatologist or traumatologist.
Upon examination, you can identify a shortened limb with a damaged joint.
The doctor will conduct an examination and prescribe a set of examinations:
- Bone densitometry to assess its density. This method allows us to evaluate the effectiveness of therapy.
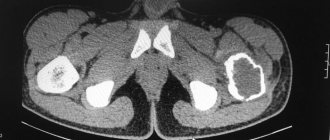
- X-ray of joints in two projections. With osteoporosis, the following signs are present on the x-ray: increased transparency of bone tissue;
- the presence of outgrowths of bone tissue in the form of spines on the articular surfaces of bones;
- fractures of bones near joints.
It is also necessary to take a blood test for
- determining the level of calcium in the blood;
- determining the level of female hormones (estrogen), thyroid hormones.
If a secondary nature of the disease is suspected, a full examination is carried out to exclude diseases leading to osteoporosis.
Stages of development of osteoporosis of the knee joint
Osteoporosis of the knee joint is characterized by 3 stages of the disease, according to which the specialist selects treatment:
- The first degree of the disease is mild and asymptomatic. It is detected together with other diseases or during a medical examination.
- The second degree is moderate. At this stage, the symptoms become more pronounced. Cartilage tissue is destroyed. Spasms bother me in the evening.
- The third degree is severe. A patient with this form of the disease is effectively disabled.
First degree
The symptoms of the disease at this stage, in contrast to grade 2 osteoporosis of the knee joint, are not pronounced. The patient may be concerned about:
- aching in the knee joint when the weather changes and high physical exertion, at this stage the destruction of the bone structure begins;
- cramps after a long walk;
- limited movement due to spasms;
- narrowing of the joint space.
Second degree
The second stage of the disease occurs with obvious symptoms, which, in comparison with grade 3 osteoporosis of the knee joint, make it possible to prescribe appropriate treatment and prevent irreversible consequences. At this stage, a person is worried about:
- cramps morning and evening;
- limited movement in the knee area;
- the occurrence of a crunch in the joint;
- joint deformation becomes visible;
- “joint mouse” syndrome, which causes severe spasms;
- The x-ray shows a strong narrowing of the joint space, bone growths are obvious.
Third degree
The third stage of the disease is the most dangerous and can cause disability. The specialist determines how to treat osteoporosis of the knee joint after identifying the following signs:
- increase in size of the joint;
- constant spasms;
- limited movement;
- change in the shape of a person’s legs;
- atrophy of the muscles near the knee;
- audible crunching sound when moving;
- X-rays show abrasion of cartilage and destruction of ligaments.
Tibial insert FREEDOM
More details
All knee replacements
Classification of endoprostheses
Materials for the manufacture of a knee joint prosthesis to replace the latter: ceramics, metal alloys, polyethylene. Depending on the design features, endoprostheses are divided into models with a movable and fixed platform.
Prostheses with a movable platform have an insert that can rotate in the metal part. This gives additional amplitude when moving the knee after surgery in the medial, lateral direction. In endoprostheses with a fixed platform, the elements - part of the tibial element and the metal component - are firmly connected to each other.
Another classification divides knee replacements into 3 types.
- Unilateral or unicondylar endoprosthesis. It is used for partial replacement of the knee joint in its upper part (prosthetic replacement of an area on one of the femoral condyles).
- Total or bilateral knee replacement (usually metal). Used to replace both parts of the joint (both femoral condyles are covered). The design of such an endoprosthesis differs from the unicondylar one in that it has more powerful attachments to the bone and increased width.
- Total endoprosthesis with axial stabilization. It is also used in total knee replacement operations, when its parts (upper and lower) are fixed with long pins along the longitudinal axes of the femur and tibia. Pins for secure fixation are driven into the space filled with bone marrow (medullary cavity).
Another sign of the classification of knee prostheses is the method of their fixation. There are 2 options: structures installed with cement and cementless methods. In the first case, when replacing a knee joint, its artificial analogue is stabilized (fixed) with quick-curing medical cement. With the cementless method, fixation is carried out as bone tissue grows into the implant.
Cemented knee joint prostheses are more reliable and versatile (used in any type of replacement surgery). An endoprosthesis for cementless installation has a special surface - porous, textured (it provides the opportunity for bone to grow into the implant).
Diffuse type of disease
The second stage of the disease is otherwise called “diffuse osteoporosis.” Typical for this stage of pathology is the appearance of malignant tumors. The bones become very thin, but are not always subject to fracture. It is diagnosed in patients over 50 years of age, but can also affect children. The causes of the disease are different:
- changes in hormonal levels;
- malfunction of the thyroid gland;
- unbalanced diet;
- heredity.
The diffuse type of the disease, as well as grade 1 osteoporosis of the knee joint, can be detected using an x-ray, which shows a noticeable thinning of the bones. Timely diagnosis can prevent bone loss.
The relationship between osteoporosis and osteoarthritis
Questions regarding the relationship between osteoarthritis (OA) and osteoporosis (OP) have been addressed since the late 1960s. Thus, surgeons during operations for hip fractures in patients with AP noted that they had virtually no signs of coxarthrosis [1]. The presence of OA protected against the occurrence of fractures in the proximal femur and spine. In clinical practice, the presence of these two diseases in one patient was considered rare [2]. Scientists have not yet come to a consensus as to whether in this case we are talking about two mutually exclusive diagnoses or not. Is the presence of OA really a protective sign for the development of AP? Today it is known that OA and AP are very common diseases of the musculoskeletal system in older people. Thus, OA accounts for more than 75% of all rheumatic diseases; it is observed in more than 50% of people aged 65 years and older, and more than 1/3 of them develop impairment of various types of physical activity. The prevalence of AP in Russia among patients aged 50 years and older is 30–33% among women and 22–24% among men. Both diseases occur in both women and men, but are more often reported in women, especially after menopause. Thus, OA is detected in every tenth woman over the age of 50, and by the age of 75 - in every second. One in three menopausal women and more than half of those aged 75–80 years suffer from AP. The social significance of AP is determined by its consequences - fractures of the vertebrae and bones of the peripheral skeleton. Among the urban population of Russia, 24% of women and 13% of men aged 50 years and older have at least one clinically significant fracture. The incidence of osteoporotic fractures increases significantly with age, and the prevalence of proximal femur fractures increases exponentially.
The number of AP and OA increases with age, therefore, the increase in life expectancy observed in recent decades in developed countries and, accordingly, the increase in the proportion of older people, especially women, in the population, leads to an increase in the frequency of these diseases, turning them into one of the most important health problems worldwide world.
Although both OA and OP are more common among people of older age groups, nevertheless, patients with these diseases have significant anthropometric differences (for example, OA usually occurs in people with increased body weight, and OP, on the contrary, in frail women), indicating that these two diseases are caused by different processes (Table) [3, 4].
Over the past 30 years, more than 40 studies have been published using various measurement techniques to examine the effects of OA on bone mineral density (BMD) in various skeletal regions. The authors of most of these studies revealed significantly higher BMD rates in patients with OA compared to the control group. However, there are studies in which no increase in BMD was found and even a decrease was noted. Contradictions in the data obtained can be attributed to differences in the selection of individuals for examination, measurement of BMD in different areas of the skeleton, the use of different measuring techniques and different methods for assessing results [2].
In 1995, the first large cross-sectional epidemiological study [5] assessed the association between radiological signs of coxarthrosis and BMD of the proximal femur and spine, measured using dual X-ray absorptiometry, in 4855 women aged 65 years and older. It was found that older white women with moderate to severe forms of radiographically evident coxarthrosis had higher BMD in all parameters compared with women without coxarthrosis, and there was a correlation of a generalized increase in BMD with bilateral coxarthrosis and severe osteophytosis.
The Rotterdam prospective study (1996) was the first to examine the relationship between radiographic OA, assessed according to the Kellgren and Lawrence criteria, BMD in the femoral neck and its dynamics, adjusted for age and body mass index (BMI). A study that involved 1,723 people who were observed for 2 years demonstrated a significant association of coxarthrosis with high BMD and an increase in BMD with disease progression [6].
In addition, studies conducted on twin women confirmed the inverse relationship between OA and OP in the proximal femur. Severe osteophytosis in the hip joint was associated with a 5–6% increase in BMD in this joint [7].
In patients with OA of the knee joints, increased BMD in the proximal femur and spine was also determined, compared with the values observed in individuals without OA [8, 9]. At the same time, a significant increase in BMD of the spine and femoral neck was shown with an increase in the stage of gonarthrosis from 1st to 4th. In addition, a prospective study demonstrated that higher BMD values increase the risk of developing radiographic knee OA [10]. In people with OA of the knee and hip joints, BMD was 3–8% higher compared to healthy study participants [6].
In case of OA of the hands, data on BMD in various areas of the skeleton are contradictory; significant deviations in BMD were not always detected, especially in the presence of isolated lesions.
According to L.I. Alekseeva and co-authors [11], in women with OP of the lumbar spine, the incidence of OA of the knee joints and nodular form was lower than in patients with normal BMD values (53.3 and 38.9%; 78.6 and 53.6%, respectively, p < 0.05). In women with OP of the femoral neck, the nodular form of OA was less frequently diagnosed compared to women with normal BMD (25.9 and 47.8%, respectively, p < 0.05). Thus, these data support the hypothesis that higher BMD is associated with OA.
Interpretation of densitometry results in spinal OA is often difficult due to the presence of osteophytes, narrowing of intervertebral discs, and sclerosis of facet joints. Thus, according to Peel et al [12], in women with spinal OA, BMD of the lumbar spine was increased by 7.9%, in the femoral neck by 6.4%, and in the whole body by 8.4%. In addition, a study of markers of bone turnover showed that in women with spinal OA aged 50–85 years, the levels of markers of both bone formation and resorption decrease, i.e., bone turnover is reduced, and therefore, the loss of BMD is less than in women of the same age without OA.
Other studies demonstrate increased bone formation, which also explains increased BMD in individuals with OA. The inconsistency of the results obtained may be due to the study of different stages of the disease. Thus, the early stages are characterized by rapid formation processes, and in the later stages there is a slowdown in bone turnover in the subchondral part of the bone, which can be considered as a secondary process in relation to the destruction of cartilage and a decrease in static load.
The social significance of AP is determined by its consequences - fractures of the vertebrae and bones of the peripheral skeleton, causing a significant increase in morbidity, disability and mortality among the elderly and, accordingly, large material costs in the field of healthcare. Therefore, the question of particular interest is: does increased BMD associated with the presence of OA lead to a reduced risk of fractures? Two population-based controlled studies of hip fractures [13, 14] showed that OA was associated with a reduced risk of hip fracture. Another study demonstrated that severe hip OA was negatively correlated with vertebral compression fractures. On the other hand, according to some data, despite a 5% increase in BMD in people with coxarthrosis, such patients have a significantly higher risk of fractures compared to the control group. The authors suggested that the increased risk of fractures in people with OA of the hip joints was most likely associated with an increased risk of falls in these patients due to impaired locomotor function of these joints. Individuals with spinal OA, however, had a lower risk of fractures, while no significant associations were found between knee OA and hand OA and fractures [15].
Subsequently, observation of a sample of elderly women, carried out for more than 7 years, showed that despite higher BMD in people with OA of the hip joints and OA of the hands, the risk of both vertebral and non-vertebral fractures, including femoral neck fractures, was not observed in such patients. decreases.
Possible mechanisms of the relationship between OA and BMD
In many clinical studies that revealed a negative relationship between OA and AP, the formation of the pathological process was influenced by obesity, race, excessive physical activity, i.e. factors that in one way or another contribute to the growth or maintenance of bone mass, but at the same time they increase the risk of developing OA. For example, obesity, a risk factor for knee OA, is associated with increased BMD. Exercise at a young age is important for achieving peak bone mass, but excessive exercise and excess weight predispose to the development of OA in later life. As is known, bone, to a greater extent than cartilage, weakens the load experienced by the joint; under increased loads it becomes denser, which creates the preconditions for the development of OA. Epidemiological studies have shown that OA is more common among Africans and people of African descent than among white people, and the prevalence of OP, on the contrary, appears to be higher among Caucasians. The reasons for these racial differences are unclear, but black individuals have higher bone mass and slower bone turnover, resulting in a higher average age of skeletal tissue.
OA is based on damage to all components of the joint, primarily cartilage, as well as subchondral bone, synovial membrane, ligaments, capsule, and periarticular muscles. In recent years, a theory has emerged that changes occurring in the subchondral bone may initiate cartilage degradation. One hypothesis is the ability of subchondral bone to produce large amounts of proinflammatory cytokines and growth factors, which can penetrate into the overlying cartilage and lead to degradation of cartilage tissue.
Little information has been accumulated on normal remodeling and turnover rates in human subchondral bone due to the difficulty of obtaining healthy bone samples. The rate of remodeling has been shown to decrease at sites subject to stress because high levels of bone tension inhibit the formation of new sites of bone turnover. A lower rate of remodeling leads to an increase in the average age of tissue in load-bearing areas and accumulation of mineral in them.
One of the main pathogenetic mechanisms for the development of primary AP is estrogen deficiency. However, some epidemiological data suggest the possible involvement of estrogens in the development of OA. Thus, OA occurs with approximately the same frequency in men and women under the age of 50, while after the onset of natural or surgical menopause there is an increase in incidence among women. There is also an association of OA with overweight and obesity, which lead to increased production of endogenous estrogens. Estrogens regulate bone turnover, and the increase in bone mass resulting from their excess creates additional mechanical stress on the cartilage during forceful impact on the joint. In addition, estrogens can cause the development of OA through cytokines and growth factors. For example, the cytokines interleukin-1 (IL-1) and tumor necrosis factor-a increase the production of enzymes that degrade the cartilage matrix. Insulin-like growth factor-1 (IGF-1) stimulates bone formation by enhancing bone cell proliferation and differentiation. Transforming growth factor-β (TGF-β) can lead to increased collagen synthesis due to its ability to stimulate the formation of osteoblasts from their precursors [16]. Since estrogens increase the concentrations of IGF-1 and TGF-β in bone tissue, increased bone formation under the influence of these factors may determine the relationship between excess weight, increased mineral density of subchondral bone tissue and the development of OA.
In addition, it has been suggested that increased bone density in OA may be achieved by reducing the level of colony-stimulating growth factor-1 (CSF-1), which stimulates osteoclastogenesis and regulates osteoclast activity. The absence of CSF-1 leads to the development of osteopetrosis in mice, and its elevated levels in the blood serum were found in individuals with AP.
In recent years, evidence has emerged that vitamin D takes part in the metabolism of not only bone, but also cartilage tissue. In particular, it has been shown that vitamin D stimulates the synthesis of proteoglycan by chondrocytes and modulates the activity of metalloproteinases involved in the destruction of cartilage. For example, a decrease in the level of 24,25(OH)2- and 1,25(OH)2-vitamin D is associated with an increase in the activity of metalloproteinases, and normalization of their level reduces the activity of these enzymes in vitro. It should also be emphasized that in the early stages of OA, vitamin D-dependent disruption of cartilage metabolism may be accompanied by remodeling and thickening of subchondral bone tissue. This leads to a decrease in the shock-absorbing capacity of the subchondral bone and acceleration of degenerative changes in the cartilage. It has been demonstrated that in patients with gonarthrosis, reduced vitamin D intake and low serum levels of 25(OH) vitamin D are associated with a 3-fold increase in the risk of progression of radiological signs of OA [3].
Vitamin D deficiency entails an increase in the synthesis of parathyroid hormone, which leads to stimulation of osteoclast activity and increased bone resorption. In addition to its effect on bone cells, in vitro studies have shown that parathyroid hormone is able to enhance the proliferation of chondrocytes in the growth plate, as well as have a dose-dependent stimulating effect on the synthesis of collagen and proteoglycans.
The above data indicate the contribution of various factors to the formation of bone tissue and the development of OA. In recent years, interest in studying the role of genetic factors in the development of OA and AP has increased. Thus, it was found that up to 80% of peak bone mass is determined genetically. The most studied gene is the vitamin D receptor (VDR) gene. Currently, there is evidence of the association of its polymorphism not only with OP, but also with OA, especially in the development of osteophytes. TGF-β gene polymorphism is also associated with AP and spinal osteophytosis. The most likely reason for the “alternative relationship” between OP and OA appears to be gene polymorphism. A study of a sample of twins showed that BMD and OA are determined mainly by genetic factors, the variability of which can determine a number of anthropometric characteristics, an increase in the synthesis of growth factors by osteoblasts and a local acceleration of bone turnover in the joint [4].
Treatment of AP is not an easy task: it must be long-term, since the effect of its use can appear after a long time. The goal of treatment is to slow down and, if possible, stop bone loss, prevent bone fractures, as well as improve the patient’s condition, reduce pain and generally improve the quality of life of patients. Pathogenetic therapy for AP includes drugs that slow down bone resorption - bisphosphonates, calcitonin, estrogens.
The drug alendronate (Fosamax), which is a nitrogen-containing bisphosphonate, is registered in Russia. In multicenter randomized, double-blind, placebo-controlled studies, alendronate at a dose of 10 mg/day showed high efficacy: increasing BMD in all areas of measurement from 5.4 to 13.7%, it significantly reduced the incidence of fractures in the spine by 47%, hip - by 51–56%, forearm - by 48%, and in 64% of patients the progression of vertebral deformities decreased. In a study of the effectiveness of alendronate at a dose of 70 mg once a week compared with 10 mg daily, it was shown that the increase in BMD was 6.8 and 7.4%, respectively, in the spine, and 4.1 and 4.3%, respectively, in the hip. However, it has been clearly shown that the tolerability of alendronate at a dose of 70 mg once a week is equivalent to taking 10 mg per day, and bone biopsy material did not reveal signs of osteomalacia at both doses of the drug. Contraindications for alendronate therapy are hypersensitivity to the drug, hypocalcemia, and the presence of esophageal diseases.
Alendronate showed a consistent therapeutic effect over 10 years of treatment. After discontinuation of alendronate therapy, patients did not experience an increase in bone density loss compared with placebo.
Alendronate is prescribed 70 mg once a week or 10 mg daily for a long time, for 3–5 years, but the exact duration has not been determined.
Positive results were also obtained in experimental studies using bisphosphonates for OA. Thus, in an experiment on a model of OA in rats with dissection of the anterior cruciate ligament, the chondroprotective effect of alendronate was confirmed, as well as its modeling effect on the subchondral bone: a decrease in resorption in the early stages after surgery and prevention of a subsequent increase in bone formation starting from the 10th week after surgery. In addition, a decrease in vascular invasion into the area of calcified cartilage and a dose-dependent inhibition of osteophyte growth were noted.
Salmon calcitonin (miacalcic) is another drug used to treat AP and prevent fractures and is available in two forms: 100 IU injection ampoules and 200 IU nasal spray bottles in 1 dose.
In accordance with the recommendations for intranasal use, the drug at a dose of 200 IU per day can be administered continuously for 3–5 years, taking into account its effectiveness, or in cyclic courses (2–3 months of treatment, 2–3 months break).
The only absolute contraindication to the use of salmon calcitonin preparations is individual hypersensitivity to the drug or its method of administration. The most common side effect of calcitonin nasal spray is irritation of the nasal mucosa. Minor nosebleeds and other nasal symptoms are less common. In most cases, these adverse reactions are mild or moderate and do not require discontinuation of the drug. With parenteral administration of calcitonin preparations, side effects are observed more often: nausea or vomiting, hot flashes to the face and skin rash at the injection site. Serious complications when using nasal or parenteral forms of calcitonin are observed in less than 1% of patients.
In recent years, work has begun to study the effect of calcitonin on the course of OA, which is associated with the possibility of interfering with the metabolism of subchondral bone, as well as the presence of chondroprotective effects.
An important component in the mechanism of action of calcitonin is its ability to exert an analgesic effect through both direct central and peripheral actions.
The positive effect of hormone replacement therapy (HRT) on the risk of fractures in postmenopausal AP has been proven. The use of HRT not only prevents bone loss in postmenopausal women, but also increases BMD in 95% of women. The increase in bone mass in the lumbar spine averages from 2 to 6% over 12 months. It was noted that the effect of HRT is higher in women with lower initial BMD and in those who had an additional risk factor for the development of AP, for example, long-term smoking. A series of multicenter studies in the United States were conducted in this direction, and in particular the WHI study (Women's Health Initiative, 2003), which included more than 16,600 postmenopausal women who received HRT for more than 5 years (8506 people) and were observed in the group placebo (8102 people). Reductions in the risk of hip fractures were observed in 34%, spine fractures in 34%, and total fractures in 24% of the treatment group. However, in the group receiving HRT, there was an increased risk of coronary heart disease, stroke, breast cancer (the maximum risk was obtained between the 4th and 5th year of the study), and thromboembolism. Due to these side effects of HRT, their long-term use for the treatment of AP is limited; the question of the prescription and duration of HRT is decided individually for each patient, depending on contraindications and the possible risk of complications.
The effect of HRT on the risk of occurrence and course of OA remains not fully understood. Thus, data from epidemiological prospective studies showed the effect of HRT in relation to the radiographic progression of OA, while their effectiveness in manifest OA of the knee and hip joints was less significant.
The preliminary results obtained on the use of anti-osteoporotic drugs for the treatment of OA indicate the need for further research to study the mechanisms of action of these drugs and develop schemes for their use.
Thus, an analysis of works devoted to the study of OA and AP showed that in OA of large joints there is an increase in BMD in all parameters, but in other forms of OA this relationship with BMD is less pronounced. There has been no reliable evidence of a reduction in the risk of fractures in patients with OA. Prospective studies have shown that higher BMD increases the risk of developing knee OA, and the mechanisms leading to the progression of OA may vary. The presence of elevated levels of growth factors in bone predisposes to cartilage degradation and protects against loss of BMD. As with AP, the development of OA depends on a whole set of genes, and the association of these diseases with different alleles of the same genes may be one of the reasons that the combined occurrence of AP and OA is quite rare.
Further study of these two widespread diseases will make it possible to carry out preventive measures aimed at reducing the risk of developing both the diseases themselves and their complications, which, in turn, lead to a decrease in both the quality and life expectancy.
Literature
- Byer PD, Contepomi CA, Farkas TA A post mortem study of the hip joint. Including the prevalence of the features of the right side//Ann. Rheum. Dis. 1970; 29(1): 15-31.
- Dequeker J. Inverse relationship osteoarthritis-osteoporosis: what is the evidence? What are the consequences?//Br. J. Rheumatol. 1996; 35: 813-820.
- Nasonov E. L. Osteoporosis and osteoarthrosis: mutually exclusive or complementary diseases? // Consilium medicum. 2000. No. 2(6). pp. 248-250.
- Alekseeva L. I. Osteoarthrosis and osteoporosis/guide to osteoporosis/ed. L. I. Benevolenskaya. M.: Binom, 2003. pp. 482-502.
- Nevitt MC, Lane NE, Scott JC, Hochberg MC, Pressman AR, Genant HK et al. Radiographic osteoarthritis of the hip and bone mineral density. The Study of Osteoporoti Fractures. Research Group//Arthritis Rheum. 1995; 38(7): 907-916.
- Burger H., van Daele PL, Odding E., Valkenburg HA, Hofman A., Grobbee DE et al. Association of radiographically evident osteoarthritis with higher bone mineral density and increased bone loss with age. The Rotterdam Study//Arthritis Rheum. 1996; 39(1): 81-86.
- Antoniades L., Macgregor A J., Matson M., Spector TD A cotwin control study of the relationship between hip osteoarthritis and bone mineral density//Arthritis Rheum 2000; 43(7): 1450-1455
- Hannan MT, Anderson JJ, Zhang Y., Levy D., Felson DT Bone mineral density and knee osteoarthritis in elderly men and women. The Framingham Study//Arthritis Rheum 1993; 36(12): 1671-1680.
- Hart DJ, Mootoosamy I., Doyle DV, Spector TD The relationship between osteoarthritis and osteoporosis in the general population: the Chigford Study//Ann. Rheum. Dis. 1994; 53(3): 158-162.
- Zhang Y., Hannan M T., Chaisson CE, McAlindon TE, Evans SR, Aliabadi P. et al. Bone mineral density and risk of incident and progressive radiographic knee osteoarthritis in women: the Framingham Study//J. Rheumatol. 2000; 27(4): 1032-1037.
- Alekseeva L. I., Benevolenskaya L. I., Mikhailov E. E., Smirnov A. V. Prevalence of osteoarthritis of the knee joints and joints of the hands among individuals with different indicators of bone mass density: Abstracts of the Third Russian Symposium on Osteoporosis. St. Petersburg, 2000. P. 78.
- Peel NFA, Barrington JA, Blumsohn A. et al. Bone mineral density ans bone turnover in spinal osteoarthritis//Ann. Rheum. Dis. 1995; 54: 867-871.
- Dequeker J., Johnell O. Osteoarthritis protects against femoral neck fracture: MEDOS study experience//Bone. 1993; 14: 51-56.
- Cumming RG, Klineberg RJ Epidemiological study of the relationship between arthritis of the hip and hip fractures//Ann. Rheum. Dis. 1993; 52: 707-710.
- Arden NK, Nevitt MC, Lane NE, Gore LR, Hochberg MC, Scott JC et al. Osteoarthritis and risk of falls, rates of bone loss, and osteoporotic fractures. Study of Osteoporotic Fractures Research Group//Arthritis. Rheum. 1999; 42(7): 1378-1385.
- Mansell JP, Bailey AJ Abnormal cancellous bone collagen metabolism in osteoarthritis//J. Clin. Invest. 1998; 101(8): 1596-1603.
N. V. Toroptsova, Candidate of Medical Sciences Institute of Rheumatology, Moscow
Signs of the disease
The disease may manifest itself with the following symptoms:
- reaction of joints to weather fluctuations;
- night cramps;
- delamination of the nail plates.
If you do not pay attention to these symptoms, the disease will gradually move to the second stage and will be characterized by:
- regular pain;
- spasms while walking;
- inflammatory processes with swelling of the knee area;
- pain when palpating the knees.
In advanced stages of the disease:
- the knee will not actually bend;
- joints increase in size.
How to diagnose
At your first visit, your doctor will examine and feel your knee joint to determine the cause of the disease. A specialist may prescribe the following procedures:
- X-ray. The images allow us to determine the presence of osteophytes and irreversible processes in cartilage.
- Absorptiometry. Examination of the knee using two x-rays, revealing bone density and the area of dangerous changes.
- Biochemistry of blood. Allows you to determine disruptions in the metabolism of calcium and hormones of the female reproductive system.
Sometimes a specialist sends a patient to undergo an MRI in order to identify the nature of changes in the bones.
Treatment options
Treatment of osteoporosis of the knee joint takes a long time. After making a diagnosis, the doctor will prescribe certain medications. Analgesics relieve pain. In addition, non-steroidal anti-inflammatory drugs are prescribed. They remove spasms and get rid of the source of inflammation. Chondroprotectors allow you to restore cartilage tissue. Sometimes intra-articular injections are prescribed. A properly formulated diet helps in the fight against the disease.
Conservative treatment methods
In the initial stages, drug treatment is highly effective. The following medications are usually prescribed:
- painkillers and anti-inflammatory drugs (Diclofenac, Ibuprofen);
- calcium-containing products;
- phytoestrogens (Dioscorea) to normalize hormonal levels;
- bisphosphonates (Bondronate, Zoledronate) – inhibit the excretion of calcium from the body.
A specialist may prescribe vitamins and hyaluronic acid injections. The substance has a softening effect and can restore the functionality of the knee joint.
Folk remedies
Folk remedies are effective at the initial stage of the disease. Prescribed as an addition to the main course of treatment:
- Compress. Mix 3 tablespoons of apple cider vinegar with one spoon of honey. Apply overnight to the affected area and wrap with burdock and then with cloth.
- Infusion. Boil one spoon of lingonberry leaves in 200 ml of water. Wait until it cools down and drink throughout the day.
Osteoporosis. Don't give him a single chance!
Drug therapy for osteoporosis has reached a fairly high level in recent years thanks to the efforts of pharmacological companies conducting active research in this area. The choice of drugs is so large that the length of the article does not allow us to talk about all the drugs, but one of them, nevertheless, is worth mentioning - Miacalcic nasal aerosol. Systematic use of this drug prevents bone destruction, increases bone density and reduces the risk of fractures. As mentioned above, calcium supplements for osteoporosis do not always need to be taken. First of all, it is necessary to take medications that help this calcium to be absorbed or suppress the process of removing calcium from the bones. The development of new drugs to combat osteoporosis is ongoing, new drugs regularly appear on the pharmacological market, but, nevertheless, nothing can replace a healthy, active lifestyle, proper nutrition and exercise. So, if you are over 50, have minor back pain and are predisposed to developing osteoporosis, do not delay visiting your doctor, take care of your health in advance. By contacting our Center, you can always count on a consultation with a highly qualified orthopedic traumatologist, the necessary research and competent treatment for osteoporosis. Say no to osteoporosis!
Prevention of osteoporosis of the knee joint
Prevention of the disease should begin at a young age. It is recommended to adhere to the following standards:
- lead an active lifestyle (biking, running, gymnastics);
- adhere to proper nutrition (food with the necessary content of calcium and minerals);
- to refuse from bad habits.
It is necessary to undergo regular bone density testing. Monitoring older patients with a doctor will eliminate the risk of fractures. Osteoporosis of the knee joint is a common disease. It will not be possible to overcome it with medications alone. Timely contact with a specialist can prevent bone destruction. Lifestyle changes and proper nutrition are the key to effective treatment of osteoporosis.
Is it possible to minimize risks?
Yes it is possible. To avoid loosening of the prosthesis after surgery, it is fixed with bone cement. And to prevent postoperative bone resorption, patients are prescribed a number of drugs. This approach minimizes the risk of fractures and postoperative instability of endoprosthetic components.
The acetabulum fracture is indicated by the blue arrow.
Knee replacement in the Czech Republic: guarantees, prices, rehabilitation, reviews and statistics.
Find out more
Minimally invasive endoprosthetics in the Czech Republic: doctors, rehabilitation, terms and prices.
Find out more