At present, unfortunately, there is no tendency to reduce the incidence of tuberculosis among the population. Ukraine continues to be among the “top ratings” in terms of tuberculosis prevalence statistics.
Quite often we come across leaflets, posters or brochures explaining what pulmonary tuberculosis is. I want to talk a little about other manifestations of this disease in humans. For example, in large joints: hip, knee, shoulder , damage to which can go undiagnosed for a long time and be masked as external manifestations of arthrosis.
Tuberculous coxitis (tuberculosis of the hip joint)
According to statistics, the most common joint affected by tuberculosis is the hip joint.
Symptoms
Tuberculous coxitis is characterized by a long-term chronic course and periodic exacerbations. An exacerbation usually occurs when the intraosseous focus of tuberculosis breaks into the joint cavity. Patients may complain of low-grade fever, weakness, fatigue, and lameness. The pain can be in both the hip and knee joints, which naturally complicates diagnosis. During an exacerbation of the disease, swelling is observed in the joint area and enlarged lymph nodes can be felt.
Diagnostics
Most often, at the initial stages, classical X-ray diagnostics are used; it is better to use digital radiography. Using the image, bone atrophy, local, and later widespread osteoporosis can be diagnosed.
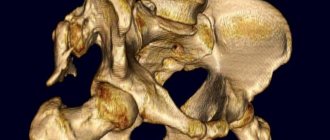
In cases where making a diagnosis may be difficult or simply requires a more detailed diagnosis and a 3-dimensional view of the lesion, spiral computed tomography (SCT) can be used.
Cases of tuberculous joint damage in children in the practice of a rheumatologist
Monoarticular lesions in children are a common joint pathology in the practice of a rheumatologist and pediatric orthopedist, requiring a wide range of differential diagnostics. It includes juvenile idiopathic arthritis, reactive arthritis, tumor process, arthritis in the structure of systemic connective tissue diseases, arthritis associated with infection. Any arthritis, especially one that does not respond to standard anti-inflammatory and antibacterial therapy, has a chronic course with a pronounced pain component or a clinical picture with radiological signs of an erosive-destructive process, should be questioned about the possible specific etiology of the process.
The modern range of examinations using ultrasound, magnetic resonance, computed tomography, direct visualization of the joint cavity using endovideosurgery and targeted biopsy increases the likelihood of a correct diagnosis. However, the relative rarity of articular tuberculous lesions, the polymorphism of clinical manifestations and the rather low coverage of phthisioosteology create the prerequisites for later diagnosis and inadequate therapy. Currently, the problem of osteoarticular tuberculosis in children is very relevant in medical practice and especially in arthrology.
According to statistics for 2009, the incidence of tuberculosis in Russia was 82 cases per 100 thousand population, while the incidence in children was about 16 cases per 100,000 children. The number of newly infected people has more than doubled over the past 10 years, and annually this amounts to 1.5–2% of the country’s total child population. And the infection rate of children living with sick people is 10 times higher than children from a healthy environment. The coverage of children with specific vaccination in the country is almost 95%, and with tuberculin diagnostics - 85%. Cases of vaccination complications with the development of BCG osteitis in children amounted to 5% in 2005 [1, 2]. According to foreign authors, the frequency of extrapulmonary forms of tuberculosis in children is 5%; in the first place among the bone form of tuberculosis is damage to the spine, followed by joints of the lower extremities. Articular damage is possible in two variants:
- with direct penetration of Koch's sticks into the joint, then this arthritis is interpreted as infectious;
- or in the variant of reactive (aseptic) arthritis with an active extra-articular tuberculosis focus (Ponce's disease).
However, cases of primary articular lesions are quite rare [3]. Scientists have identified a genetic predisposition to the development of tuberculous lymphadenitis - this is a deficiency of interleukin-12/interferon-gamma system [4]. A specific tuberculosis process can develop in bones that have a good blood supply, rich in spongy substance: vertebral bodies and metaphysis, epiphyses of long tubular bones, due to rich microcirculation, slow blood flow and intimate arrangement of vessels and tissue. The onset of tuberculous lesions occurs with the formation of granulomas in the synovial membrane or the bone itself; the initial lesion of the metaphysis in the region of the growth zone is typical; radiographically it looks like local destruction with an area of demineralization. Cartilage tissue is resistant to tuberculosis, however, chronic inflammation, damage to the underlying bone tissue with malnutrition and penetration of the focus of destruction lead to damage to the cartilage shell. Articular cartilage has been a barrier to the spread of bone tuberculosis for a long time. [5]. Damage to the bone tissue itself occurs in three stages: the prearthritic phase is accompanied by the formation and development of osteitis, the arthritic phase by the clinical, laboratory and radiological picture of a specific lesion, and the third phase by the resolution or formation of anatomical and functional changes.
At the Scientific Research Institute for Children's Orthopedics. G.I. Turner, St. Petersburg, from 2000 to 2010, seven cases of the osteoarticular form of tuberculosis in children were identified. All cases were verified at the specialized rheumatology department of the institute, where patients were examined for chronic monoarthritis. In five children the disease occurred with damage to the osteochondral part of the joint, in two with soft tissue damage in the form of hygroma or bursitis. The mask of tuberculosis in the first case was the picture of chronic juvenile arthritis, an oligoarthritic variant with an exudative-proliferative component, with the formation of persistent pain contracture and paraclinical activity. At the outpatient stage, these children received monotherapy with nonsteroidal anti-inflammatory drugs (NSAIDs), one child received sulfasalazine. The soft tissue lesion in one child clinically corresponded to hygroma of the popliteal region, in the other - to infrapatellar bursitis and was accompanied by weak inflammatory activity.
All children were vaccinated with BCG in the maternity hospital, with the formation of a scar at the injection site of 3–5 mm; four children lived in an endemic region for tuberculosis pathology or had close relatives with tuberculosis. Epidemiological anamnesis denied direct contact of children with tuberculosis patients. The age of the osteochondral defect in children at the time of detection of tuberculosis was on average 2–3 years, while the duration of the disease (based on the appearance of clinical symptoms) ranged from two to four months. Thus, we can talk about a certain “silent” period. In the case of soft tissue lesions, the age of the children was 1.3 months and 11 years, and the duration of the disease was no more than 6 months. When assessing the dynamics of tuberculin tests using the Mantoux test with 2TE and analyzing the anamnesis, only one child had a change in tuberculin tests, with previous persistent focal right-sided pneumonia and a subsequent 3-month course of specific therapy with ftivazid. But the debut of the actual bone lesion in this child developed only four years later. The rest of the children, according to the results of the Mantoux test with 2TE, are only tubercularly infected.
The diagnosis of tuberculous lesions of bone tissue was suspected based on the results of an X-ray examination, including computed tomography, based on a specific pattern of lesions with the formation of foci of destruction, periosteal reaction, followed by confirmation by bacteriological and histological data. The diagnosis of soft tissue lesions was suspected during surgical resection of the hygroma on the basis of cheesy discharge from the lesion and subsequent histological visualization of the picture of tuberculous pathology.
According to the examination, three out of five children with the bone form of tuberculosis were diagnosed with “BCG-ostitis”, the onset of the disease was before three years from the time of vaccination, the course was accompanied by a clinical picture of arthritis in the first case of the ankle, in the second case of the knee, and in the third child - of the hip joint without dynamics against the background of standard NSAID therapy. In the first case, the lesion was located in the calcaneus with inflammation spreading to the ankle joint, with an area of hyperemia above the area of destruction without concomitant paraclinical activity. Tuberculous gonitis was characterized by damage to the distal epiphysis of the femur with a clinical picture of exudative-proliferative gonitis with activity II–III degrees (ESR 60 mm/h, C-reactive protein 35 mg/l), and tuberculous coxitis by damage to the head and proximal femur, clinically manifested by lameness , minimal pain and the formation of combined contracture with limitation of movements by a maximum of 10 ° C, paraclinical activity of the second degree exclusively at the onset of the disease (ESR 47 mm/h). At the same time, the ultrasound picture does not always detect the bone destructive component, and exudation, infiltration and hypervascularization are not so specific.
In another case, tuberculosis lesions of the knee joint were detected in a child of senior preschool age living in an endemic area for tuberculosis pathology. The onset of the disease is at the age of 5 with the appearance of clinical symptoms of reactive arthritis of the right knee joint, without an obvious provoking factor, accompanied by grade II activity (ESR 30 mm/h). He was examined in the pediatric department at the place of residence, the current gonitis was assessed as a part of juvenile chronic arthritis, and sulfasalazine was prescribed at the rate of 30 mg/kg/day, despite the existing radiological findings. During examination at the Scientific Research Institute for Children's Orthopedics named after. G.I. Turner, four months from the onset of the disease, a specific radiological picture of the lesion was revealed. Clinically, the articular syndrome is represented by defiguration of the right knee joint due to the exudative-proliferative component, with the formation of combined contracture and moderate muscle wasting. Laboratory findings: moderate dysproteinemia due to the alpha2 fraction, moderate thrombocytosis, acceleration of ESR to 30 mm/h.
A feature of soft tissue tuberculous lesions of the joint is the ability to clinically manifest itself under the “mask” of hygroma or chronic bursitis. Occurring without concomitant pain joint syndrome with minimal paraclinical activity, the absence of a specific x-ray and ultrasound picture, as well as a concomitant anamnesis, this form of tuberculosis seems to be the most difficult to diagnose. Over a 10-year observation period, two cases of soft tissue tuberculosis of the joint were identified in the department. For the first time, palpable formations in the knee joint area were discovered by parents by chance without an obvious provoking factor or accompanying pain syndrome. Clinically, a dense elastic formation was determined, moderately painful to the touch, not fused with the surrounding tissues, with moderate swelling of the surrounding tissues, there was no obvious articular syndrome. Radiologically, no bone-destructive changes were detected; there was isolated soft tissue compaction in the hygroma area.
There is no data on the ultrasound picture of hygroma in the popliteal region; rheovasography determined increased blood flow in the popliteal region; in the second case, infrapatellar bursitis was described with an oval-shaped formation, with clear contours, isoechoic content and without pathological vascularization. The course of hygroma of the popliteal region was accompanied by laboratory paraclinical activity of the first degree (ESR 18 mm/h); in chronic infrapatellar bursitis there was no paraclinical activity. During surgical resection of the hygroma, a section of infiltrated tissue measuring 3 × 3.5 cm with liquid discharge and fine-grained inclusions was discovered in an atypical place in the popliteal region. During inspection of the infrapatellar region, a pathological formation was discovered, covered with a capsule with milky-gray curdled contents. Histologically, in the first case, a tuberculous focus of caseous necrosis of the lymph node was confirmed, in the second, morphological changes were described (foci of caseous necrosis surrounded by a shaft of epithelial cells, lymphocytes, plasma cells, in places with the presence of varying numbers of giant multinucleated Langhans cells) observed in BCGitis.
Thus, over the 10-year period of work of the department, seven cases of the osteoarticular form of tuberculosis in children were identified, of which five cases affected the bone and two the soft tissue component of the joint. All children were transferred to a specialized hospital, where the diagnosis of tuberculosis was confirmed by histological and bacteriological methods.
In modern conditions, more and more data are accumulating indicating the possibility of the tuberculosis process occurring under the guise of chronic arthritis. The described cases of tuberculosis in children confirm the need for vigilance and a clear understanding of the pathological inflammatory process in the joint. A negative tuberculosis history, normergic Mantoux tests with 2TE, the absence of a bone destructive process, and even laboratory inflammatory activity do not exclude the course of the tuberculosis process, including damage to the soft tissue component. A pediatric rheumatologist, as well as a pediatric orthopedist, must constantly maintain a high index of suspicion regarding tuberculosis pathology.
Literature
- Infectious morbidity in the Russian Federation for January-September 2009. Federal Service for Supervision of Consumer Rights Protection and Human Welfare.
- Aksenova V. Stably severe... Medical newspaper No. 21 of March 23, 2007
- Rajakumar D., Rosenberg AM Mycobacterium tuberculosis monoarthritis in a child // Pediatric Rheumatology. 2008, 6:15.
- Francis Serour et al. Analysis of the interleukin-12/interferon-g pathway in children with non-tuberculous mycobacterial cervical lymphadenitis // European Journal of Pediatrics. Vol. 166, No. 8, August 2007.
- Tuli SM Tuberculosis of the Skeletal System: Bones, Joints, Spine 2004.
M. F. Dubko*, Candidate of Medical Sciences, Associate Professor G. A. Novik*, Doctor of Medical Sciences, Professor N. A. Pozdeeva**, Candidate of Medical Sciences A. N. Kozhevnikov* V. V. Selizov**
* SPGPMA, **Research Institute of Children's Orthopedics and Traumatology named after. G. I. Turner , St. Petersburg
Contact information for authors for correspondence
Tuberculosis drives (tuberculosis of the knee joint)
The knee joint is immediately behind the hip joint in terms of incidence according to observations.
Symptoms
There is also a temperature of about 37 degrees, fatigue, lameness, pain that increases during loads on the leg, thickening of the skin fold, swelling of the joint, and limitation of its function. A fistulous tract may even form behind the joint, in the popliteal fossa.
Diagnostics
When using classical x-rays, it is also possible to observe atrophy of the bones that form the knee joint, and uneven osteoporosis can be determined. A detailed study can reveal a lesion in the bone that grows towards the joint, followed by destruction of the articular surface.
The use of SCT immediately answers many questions of interest: the exact number of lesions, their size, structure and content, the presence of small lesions not visible on x-rays, a 3D view of the location of lesions in the bones around the joint.
Tuberculosis: causes and etiology of the disease
Tuberculosis is an infectious disease of humans and animals caused by various mycobacteria from the Mycobacterium tuberculosis complex group (Koch bacillus). Infection with these bacteria is quite widespread, especially among residents of megacities: Koch bacilli can live in street and house dust for up to 1 year, and in heat, high humidity and without light for more than 5 years. Theoretically, almost every person can be a carrier of mycobacteria, but normally the human immune system is able to suppress the infection. The disease develops with low immune status. People are the main carrier of tuberculosis bacteria, and internal organs, and especially the lungs, are a favorable environment.
Today, only 5-10% of those infected will develop tuberculosis during their lifetime. The risk increases if the patient has a history of:
- Diabetes;
- Stomach ulcer;
- HIV infection.
Tuberculosis most often affects people who smoke and drink, children and adolescents. The disease also develops in difficult social conditions, during overwork, stress, and unemployment.
Microscopic droplets of liquid with Koch rods can be present and circulate with the air in the room. In this regard, the disease is easily transmitted by airborne droplets. Patients with tuberculosis cavities in the lungs are especially contagious, since the viral load on the body of such patients is especially high. But the infectiousness of tuberculosis also varies depending on the specific type of pathogen (some strains of M. tuberculosis are considered the most dangerous) and the stage of infection.
Doctors distinguish three stages of tuberculosis:
- Primary;
- Latent;
- Active.
Tuberculosis is not transmitted at the primary stage. Bacilli of the species M. tuberculosis provoke the development of tuberculosis, which occurs predominantly in the latent stage - without acute and pronounced symptoms. Sometimes in the second stage the patient develops a cough, low-grade fever, and fever. However, the infectivity of tuberculosis decreases rapidly within 14 days of starting effective treatment.
The immune system of the human body begins to suppress their growth only 3 weeks after infection and active reproduction of mycobacteria. This happens before clinical symptoms of the disease appear. However, at this time, granulomas with caseous and necrotic foci form in the lungs. In this form, tuberculosis can live in the human body for years.
According to WHO experts, on average, each untreated patient can infect 10 to 15 people within
Types of pulmonary tuberculosis: CT picture
A CT scan of the lungs does not show a specific causative agent of tuberculosis infection from the class of mycobacteria, but it shows changes in the lungs that are not visible on conventional x-rays or fluorography due to the relatively low resolution of the latter, incomplete review, and the shadow effect that distorts diagnostic results.
Based on a specific CT image, radiologists determine the following types of tuberculosis:
- Tuberculosis of the intrathoracic lymph nodes (pulmonary root infiltration syndrome and polycyclically altered pulmonary root syndrome) is a bacterial infection of the lymph nodes of the chest and mediastinum, but there is no damage to the lungs.
- Miliary tuberculosis (miliary dissemination syndrome) is characterized by the presence of multiple millet-like tubercles in the lungs, located relatively evenly.
- Disseminated pulmonary tuberculosis - multiple foci of tuberculosis in both lungs have different sizes and are located diffusely.
- Focal tuberculosis - characterized by the presence of single or multiple foci up to 1 cm in diameter. If there are several foci, then they are located in one place.
- Infiltrative pulmonary tuberculosis - characterized by the presence of broncho-pneumonic inflammation, the formation of an area of infiltration of lung tissue more than 1 cm in diameter.
- Cavernous pulmonary tuberculosis is characterized by the formation of a cavity of destruction, disintegration of lung tissue as a result of an advanced infectious process, the so-called round or oval cavity.
- Fibrous-cavernous tuberculosis - along with cavities in the lungs, there are signs of fibrosis, which is an aggressive response of the body to inflammation and deforms the lung matrix; tuberculous scars are formed in the lungs).
The disease can occur in acute or chronic form.
The primary tuberculosis complex (early stage of the disease) is characterized by the presence of a lesion or a group of them in the lungs and enlarged lymph nodes. On a CT scan, compactions are visualized in the lobes of the lungs on one or, most often, on both sides; they are comparatively lighter in color than the entire pulmonary parenchyma and have a specific shape that is different from the pulmonary matrix, vessels and bronchi.
Annual preventive fluorography is a quick, affordable and, of course, useful examination. But this radiographic method, invented in the first half of the 20th century, is most likely to show tuberculosis “in general” and at later stages. Therefore, screening low-dose CT of the lungs (MDCT of the lungs) is considered the more preferable method for diagnosing tuberculosis today.