The base of the pelvis is the ischium, pubis and ilium. The ischium is located in the posterior lower part of the acetabulum. A thickened branch (ischial tuberosity) extends from its body; the lower part is connected to the pubic bone.
The anatomical structure is associated with cases of serious injuries to the pelvic bones that are often encountered in medical practice.
Sharp muscle contractions, blows, falls and bruises in the area of the tubercle lead to a fracture of the ischium, as well as the tubercle itself, and serious damage to various pelvic bones.
Injuries not only lead to disruption of the structure of bone tissue, but can also damage the organs located here (female internal organs, bladder, rectum).
Anatomy of the ischium
The ischium, combined with the pubis and ilium, form the pelvis, the largest pelvic bone in the human body. In an adult, these segments grow tightly together in the area of the acetabulum, the place to which the femur is attached to form the hip joint.
The ischium is located at the base of the spine, and in its anatomical structure there are 2 main parts:
- body - takes part in the formation of the acetabulum;
- branch - connects with the opposite one at an angle, forming the ischial tuberosity.
The pelvic bones are a reservoir for internal organs. They are durable, so cases of their fractures are diagnosed less frequently than injuries to long bones. Damage poses a danger to human life, since there is always a risk of rupture of the intestine with sharp bone fragments.
Structure and functions
In people under the age of 16, experts anatomically divide the pelvic bone into three separate parts - pubis, ischium, ilium. When a person reaches 16 years of age, they fuse together with the pelvic region through cartilage. This is how the pelvic ring is formed, which represents the boundary of the small and large pelvis. Gradually this connection disappears. Already at 20-21 years old, ossification can be observed almost completely.
The pelvis is located at the base of the body. He is an important part of it. The sacrum is the end of the spinal column. This bone is a kind of protective shell for human organs, which are concentrated in the buttocks area - in the small pelvis. The lower limbs are also attached there.
The acetabulum is involved in the formation of the hip joint, where the ischium is located. It is represented by two components - the body and branches that go to the pubic bones. One of the important elements of the bone is the protrusion or ischial tuberosity. The branches and body form the obturator foramen, through which vital neurovascular bundles pass.
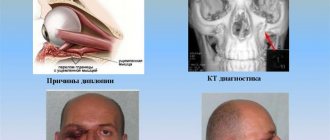
Causes of fractures
A fracture of the ischium is a serious injury that is difficult to sustain in everyday life. The human pelvis is very strong and can withstand significant loads. However, the pelvic bones can also be damaged if the mechanical pressure on them is not calculated. The most common causes of fractures include:
- an unfortunate fall on the buttocks, especially on ice or another hard surface;
- excessive compression of the pelvic bones;
- Road accident with increased pressure or impact to the pelvic area;
- sports-related injuries.
Depending on the nature of the injury, a fracture of the ischium may be stable or unstable. In the first case, the anatomical structure of the pelvic ring remains unchanged - it is a structure formed by the pelvic bones (including the ischium, pubis and ilium) and the sacrum. Unstable fractures occur with a violation of the integrity of the pelvic ring, and therefore are more dangerous for humans. Fragments of the ischium can change their location with any movement in the hip joint, after which they injure internal organs.
With offset
With unstable fractures, a person most often develops dangerous consequences. This is due to the fact that such an injury is not stable, i.e. at any moment the broken parts of the bone can move further away from each other. Moreover, their distance occurs at the slightest load.
Also, such injuries occur with active movements of the lower limbs and strong forward bending.
The peculiarity of this injury is that the pelvic ring, consisting of the sacrum and the bodies of 3 bones, is disrupted. It will take a very long time to recover from such an injury.
Classification and symptoms
Symptoms of ischium fractures vary depending on the nature of the fracture. The injury is rarely isolated; more often it occurs in combination with large-scale soft tissue damage. However, there are certain signs that indicate a fracture of this particular structure.
The ischium is one of the components of the pelvic bone, along with the pubis and ilium.
If the ischium fracture is stable, localized on one side on a bone that does not participate in the formation of the pelvic ring:
- local soreness;
- swelling of the tissue around the fracture site;
- “stuck heel” syndrome - when lying on your back, it is impossible to raise your leg straight at the knee joint.
A unilateral or bilateral fracture of the ischium, which takes part in the formation of the pelvic ring, may also occur. Identical symptoms occur when the ischium is damaged on one side and the pubis on the other:
- the presence of a local focus of pain, which increases when trying to turn or lie on one side;
- positive reaction to the sticky heel test.
The most severe clinical picture occurs in those patients who have a broken ischium with disruption of the integrity of the pelvic ring. This injury can be identified by a number of characteristic symptoms:
- acute pain in and around the fracture area;
- positive response to stuck heel syndrome;
- the patient is forced to be in a position where his legs are bent at the knee joints and moved to the sides (frog pose).
More detailed diagnostics are carried out using instrumental methods. The most common diagnosis is closed fractures of the ischium. The fragments do not change location, so treatment is quick and without consequences. When the ischium is fractured without displacement, the internal organs are not injured if the victim does not make sudden movements and aggravate the situation.
Department of Traumatology and Orthopedics
article in PDF format
DOI: 10.17238/issn2226-2016.2018.3.46-52 UDC 617-089.844 © Solod E.I., Lazarev A.F., Ovcharenko A.V., 2018
E.I. Malt1, A, A.F. Lazarev1, B, A.V. Ovcharenko2,C
1FGBU NMITsTO im. N.N. Priorov, Moscow, 127299, Russia 2BSMP im. Shevchenko, Kaluga, 248000, Russia
Abstract: In the work, the authors present the experience of using minimally invasive technologies for osteosynthesis of fractures of the acetabulum and pelvis in 84 patients from 2003 to 2021. The age of the patients ranged from 17 to 70 years. For osteosynthesis, the authors used cannulated screws and threaded wires. The authors identified indications for the use of minimally invasive osteosynthesis of pelvic fractures. Minimally invasive fixation of acetabular fractures in the early stages after injury is technically less complex and traumatic, ensures the prevention of aseptic necrosis of the femoral head and creates favorable conditions for fracture healing.
Key words: minimally invasive osteosynthesis; acetabular fractures; pelvic bone fractures; cannulated screw; threaded knitting needle; aseptic necrosis of the femoral head.
THE POSSIBILITIES OF TREATING PATIENTS WITH PELVIC INJURIES
Solod EI1,A, Lazarev AF1,B, Ovcharenko AV2,Cc
1National Medical Research Center of Traumatology and Orthopedics, Moscow, 127299, Russia 2Center for Traumatology and Orthopedics, Kaluga, 248000, Russia
summary: In the work the authors presented the experience of using minimally invasive technologies in the osteosynthesis of acetabular and pelvic fractures in 84 patients between 2003 and 2021. The age of the patients ranged from 17 to 70 years. For the osteosynthesis the authors used cannulated screws and cutting threads. The authors defined indications for the use of minimally invasive osteosynthesis of pelvic fractures. Minimally invasive fixation of acetabular fractures in early terms from the moment of trauma is technically less complicated and traumatic, it provides prevention of aseptic necrosis of the femoral head and creates favorable conditions for healing of fractures.
key words: minimally invasive osteosynthesis; acetabular fractures; fractures of pelvic bones; cannulated screw; cutting thread; aseptic necrosis of the head of the femur.
Until now, the treatment of pelvic fractures remains an urgent problem in traumatology. The most common causes of severe pelvic fractures are road traffic accidents (57%), pedestrian collisions (18%), motorcycle accidents (9%) and catatrauma (4%). Due to the constant increase in the number of vehicles, increasing speed of movement, and urbanization of life, the nature of injuries is changing with an annual increase in the proportion of multiple and combined injuries, while there is an absolute increase in the number of victims with unstable injuries of the pelvis and acetabulum.
In Russian-language literature, with rare exceptions, the term “pelvis” means a single structure. In the orthopedic and traumatological literature of the West, the concept of the pelvis identifies two anatomical and physiological formations - the pelvic ring and the acetabulum, since they differ from each other in the mechanism of injury, the characteristics of clinical and radiological diagnosis, the severity of combined injuries, survival and orthopedic prognosis. Only the last criterion for injuries of the acetabulum is more serious than for injuries of the pelvic ring, because here the gliding apparatus is disrupted, which after an injury does not tend to reverse development. That is why acetabular surgery can be classified as a separate field.
When assessing the results of surgical treatment, it was noted that a large proportion of excellent and good results were found after surgical treatment of patients with injuries of the pelvic ring (81.2%), with fractures of the acetabulum there were significantly fewer good results and they were observed in 57.1% of patients. In the long-term period after open reduction and osteosynthesis of the acetabulum, many authors note such problems as aseptic necrosis of the femoral head, lysis of fragments or heterotopic ossification, deforming arthrosis of the hip joint, which manifests itself within a year after surgery. If we consider that with open reduction of acetabular fractures there are often complications such as significant blood loss, sciatic nerve neuropathy and inflammation, then the relevance of this problem becomes clear.
This situation leads to the need to search for new methods of surgical treatment of the acetabulum and pelvis, which open up the possibility of reducing the likelihood of the occurrence of these problems and complications.
Between 2003 and 2021. in the first traumatology department of the Federal State Budgetary Institution CITO named after. N.N. Priorov performed 84 operations of minimally invasive osteosynthesis of acetabular fractures. The age of the patients ranged from 17 to 70 years. Osteosynthesis of the posterior column of the acetabulum was performed in 9 patients (14%), the anterior column in 12 patients (19%), and both columns in 43 patients (67%). Among them, the number of patients with isolated acetabular trauma was 21 (33%), multiple 23 (36%), combined 20 (31%). Primary operations for restoration of the acetabulum were performed within 1 to 3 weeks after the injury.
Clinical, radiological, electrophysiological, biomechanical and statistical research methods were used.
Long-term treatment results were assessed using the Harris scale, which included assessment of pain, function, deformity, and range of motion.
During percutaneous osteosynthesis of the acetabulum, cannulated screws “Synthes” AO 7.3 mm with a partial thread of 16 mm, pelvic screws “Synthes” AO 4.5 mm, and also wires with a diameter of 2 mm with a threaded end were used as fracture fixators.
Osteosynthesis was performed after closed reposition of fragments or reposition through minimal technological approaches using a pelvic set of reduction instruments. Metal fixators were carried out under the control of an X-ray electron optical converter (EOC) through skin punctures. The absence of blood loss made it possible to perform simultaneous osteosynthesis of extrapelvic injuries. In the postoperative period, not a single case of inflammatory complications or the development of sciatic nerve neuropathy was noted. The duration of the operation depended on the complexity of the reposition and ranged from 20 to 40 minutes.
Percutaneous osteosynthesis of both columns of the acetabulum was carried out as follows: after achieving satisfactory contact of the fragments, under the control of an image intensifier (in a mixed mode of graphing and copying) from the apex of the ischial tuberosity through the descending branch of the ischium, through the fracture line outside the cavity of the hip joint, a 2 mm threaded pin was passed end into the body of the ilium. The required length of the compression screw was determined from the spoke. After puncture of the skin (up to 1 cm) along the wire with a cannulated drill, a channel was formed. A screw (7.3 mm in diameter with an incomplete thread) of a previously determined length was tightened along the wire until interfragmental compression was achieved, which was determined radiographically by the elimination of diastasis and closure of bone fragments.
The next stage is also closed under the control of an image intensifier from a point 2 cm above the level of the acetabulum through the body under
ilium and the fracture line, a 2 mm wire was inserted into the body of the horizontal branch of the pubic bone. The required length of the screw was measured. Through a skin puncture (up to 1 cm), a self-tapping screw with a diameter of 4.5 mm was inserted into the body of the pubic bone through a channel formed by a wire. The screw was tightened until interfragmental compression was achieved, which was determined radiographically by the elimination of diastasis with closure of bone fragments.
Control of the placement of pins and screws, assessment of the quality of reposition and fixation was carried out using standard (direct, caudal, obturator, iliac) and modified combined projections.
The next day after surgery, the patients sat up in bed and began activity with crutches without full axial load on the lower limb. Postoperative management was active from the first day; the only limitation with a full range of active movements was the load on the operated limb in case of an isolated injury to the acetabulum; in the presence of extrapelvic skeletal injuries, the orthopedic regimen was selected individually.
Patient S., 48 years old, was injured in an accident on April 10, 2011. Displaced fracture of both columns of the right acetabulum. Fracture of the left ilium wing. (Fig. 1-2)
On the 5th day after the injury, percutaneous osteosynthesis of the right acetabulum was performed with a cannulated screw, a threaded wire, and the left iliac wing with a threaded wire (Fig. 3-4). The patient was activated on the first day after surgery (Fig. 5).
From the first day after surgery, exercise therapy was prescribed to maintain range of motion in the right hip joint and muscle tone of the limb. 12 days after the operation, the wounds healed by primary intention, and the patient was discharged for outpatient treatment. Dosed loads are allowed after 6 months, full loads after 8 months after surgery.
2 years after the operation, control photographs showed complete healing of the fractures, restoration of congruence of the acetabulum, and no signs of aseptic necrosis of the head.
After removal of the metal fixators (Fig. 7), the patient walks with full weight-bearing from the first day after surgery, the range of motion in the right hip joint is full (Fig. 8-9).
Patient S., 21 years old, was injured in a road accident on June 13, 2007. Combined injury. CCI. SHM, subdural hematoma, hemorrhage on the left. Fracture of both columns of the left acetabulum (Fig. 10-11).
On the 14th day from the moment of injury, after stabilization of the condition, percutaneous osteosynthesis of both columns of the left acetabulum was performed using the method described above (Fig. 12). Activated on the first day after surgery without axial load on the left lower limb (Fig. 13).
On the 12th day after surgery, the sutures were removed and he was discharged for outpatient treatment in satisfactory condition. Walking with crutches without load on the operated joint lasted 6 months after surgery, full weight-bearing without additional support was allowed after 8 months. A dosed increase in load over 2 months promotes gradual structural adaptation of the osteochondral formations of the hip joint to physiological loads after fracture healing.
A year after the operation, the patient walks with full weight-bearing, without additional support, the range of motion in the left hip joint is full, radiological signs of healed fractures (Fig. 14-15).
The presence of the metal structure did not bother the patient in any way and did not interfere with the function of the joint. After 4 years, I was admitted to the department with a fracture of the ulna (another traffic accident), and, simultaneously with osteosynthesis of the ulna, the metal structure was removed from the acetabulum (Fig. 15, 16).
Complete medical and social rehabilitation of the patient has been achieved, he walks with full weight-bearing, there is full range of movement in the left hip joint, there are no complaints.
results
When assessing the results of treatment of victims, the degree of restoration of the function of the hip joint and limbs, the number of early complications and long-term consequences were assessed. In the process of dynamic observation, we distinguished three periods: early postoperative - up to 14 days from the moment of surgery, medium-term 6 months or more from the moment of surgery, and long-term - from a year or more. In the early period, the use of minimally invasive technologies made it possible to activate patients in the study group 1-2 days after surgery and begin exercise therapy, regardless of the severity of the fractures. In two cases of severe combined injury, inflammatory complications occurred, the foci of which were not associated with postoperative wounds from percutaneous osteosynthesis.
Long-term results over a period of 1 to 10 years were monitored in 42 patients. The results were assessed using the Harris scale, with an average score of 85.5 points. The pain syndrome did not bother me, the patients were medically and socially rehabilitated. Aseptic necrosis of the femoral head was detected in 4 patients after 5 years, which accounted for 19% of cases. All these patients underwent hip replacement. In this case, the operation was performed without technical difficulties, since the anatomy of the acetabulum was minimally changed and the metal structures did not interfere with surgical manipulations, in contrast to cases of endoprosthetics after open osteosynthesis.
In all cases, as a result of treatment, functional fitness of the lower extremities was achieved. Excellent and good results of percutaneous osteosynthesis for fractures of the acetabulum persist in the medium term for up to 10 years.
Discussion
Taking into account the anatomical and biomechanical features of acetabular injuries has an objective impact on the formation of treatment tactics, which contributes to a faster and more complete recovery after injury and improved quality of life in the future. The first point of classification is the division of all patients into two large groups: A – isolated injuries of the acetabulum (segment 62 according to the International Classification of Fractures AO) and B – in combination with damage to the pelvic ring (segment 61). this is essential in determining the volume and timing of treatment measures [10,11[.
The main criterion for choosing surgical tactics is the preservation of the blood supply to the femoral head and acetabulum, as well as the possibility of restoring congruence of the hip joint without transarticular access.
It is very important to estimate what percentage of the roof remains intact to understand the degree of stability of the femoral head in the acetabulum (12). According to Matta et al., if the angle of the acetabular roof arch is less than 45 degrees, then the patient should be operated on to restore the stability of the femoral head.
Factors influencing the fate of the joint include subluxation of the femoral head, the degree of destruction of the cartilaginous surfaces of the acetabulum and femoral head, and the presence of intra-articular fragments.
Fractures in the load-bearing area are subject to mandatory surgical treatment. The only exception may be comminuted fractures of both columns. In such situations, congruence in the joint can be restored a second time. A very small number of socket roof fractures can be treated conservatively. Large fragments of the posterior wall lead to instability of the femoral head and require fixation. Destruction of more than half of the posterior wall of the acetabulum creates new conditions for instability [13,14].
Calkins et al. According to computed tomography data, it was revealed that if 34% of the articular surface of the posterior wall of the acetabulum remains intact, the joint becomes unstable. If 55% of the posterior wall is preserved, the joint remains stable. Tornetta showed in an experiment that relatively stable options become unstable under axial load.
On oblique projections through the obturator foramen, the degree of displacement is clearly visible. The displacement test is easier to check with the hip joint flexed at 90 degrees under the control of an image intensifier.
All cases of unreduced fracture-dislocations with conservative treatment, fractures of the posterior edge with a large (more than 2 cm) fragment, interposition of fragments in the joint, T-shaped fractures of the floor of the acetabulum are subject to surgical treatment.
Open reduction and internal fixation is a common treatment for displaced acetabular fractures. However, not all patients are good candidates for this procedure. Tile oezda travmatologov-ortopedov Rossii. 2010. P. 38]
11. Zamzam MM Unstable pelvic ring injuries. Outcome and timing of surgical treatment by internal fixation / MM Zamzan // Saudi Med.J. – 2004. – Vol. 25, N 11. – P. 1670 – 1674.
12. Matta JM, Anderson LM, Epstein HC, et al: Fractures of the acetabulum. A retrospective analysis.// Clin Orthop Relat Res 205:230-40, 1986.
13. Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum: a meta-analysis // J Bone Joint Surg [Br] 2005;87:2–9.
14. Matta JM, Mehne DK, Roffi R. Fractures of the acetabulum: early results of a prospective study // Clin Orthop 1986;205:241–50
15. Tile M, Helfet D, Kellam J. Fractures of the pelvis and acetabulum // 3rd ed., Baltimore: Lippincott, wilkins and williams; 2003.
16. Letounel E, Judet R. Fractures of the acetabulum // 2nd ed., Berlin: Springer Verlag; 1993.
17. JL Gary et al. Survivorship of the native hip joint after percutaneous
repair of acetabular fractures in the elderly. // Injury, Int. J. Care Injured 42 (2011) 1144–1151 DOI: 10.1016/j.injury.2010.08.035
18. Mouhsine E, Garofalo R, Borens O, et al. Percutaneous retrograde screwing for stabilization of acetabular fractures// Injury 2005;36:1330– 6. DOI: 10.1016/j.injury.2004.09.016
19. Starr AJ, Jones AL, Reinert CM, Borer DS. Preliminary results and com-plications following limited open reduction and percutaneous screw fixation of displaced fractures of the acetabulum// Injury 2001;32:45–50.
20. Gay SB, Sistrom C, Wang GJ et al. Percutaneous screw fixation of acetabular fractures with CT guidance: preliminary results of a new technique// AJR Am J Roentgenol 1992;158:819–22. DOI: 10.2214/ajr.158.4.1546599
21. Routt ML, Simonia PT, Grujic L. The retrograde medullary superior pubic ramus screw for the treatment of anterior pelvic ring disruptions: a new technique // J Orthop Trauma 1995;9:35–44.
22. Attias N, Lindsey RW, Starr AJ et al. The use of a virtual three-dimensional model to evaluate the intraosseous space available for percutaneous screw fixation of acetabular fractures // J Bone Joint Surg [Br] 2005;87:1520–3. DOI: 10.1302/0301-620x.87B11.16614
23. Chen et al. Differences of percutaneous retrograde screw fixation of anterior column acetabular fractures between male and female: A study of 164 virtual three-dimensional models // Injury, Int. J. Care Injured 40 (2009) 1067–1072 DOI: 10.1016/j.injury.2009.01.014
24. Rommens PM. Is there a role for percutaneous pelvic and acetabular reconstruction// Injury 2007;38:463–77 DOI: 10.1016/j.injury.2007.01.025
25. Starr AJ, Reinert CM, Jones AL. Percutaneous fixation of the columns of the acetabulum: a new technique // J Orthop Trauma 1998;12(1):51-8.
26. Mears DS, Velyvis JH Primary total hip arthroplasty after acetabular fracture // J. Bone Jt Surgery. – 2000. – V. 82. – P. 1328.
27. Bellabarba C, Berger RA, Bentley CD, et al. Cementless acetabular reconstruction after acetabular fracture // J Bone Joint Surg Am 2001;83:868–76.
Author information
Solod Eduard Ivanovich – Doctor of Medical Sciences, Senior Researcher first branch of the National Medical Research Center for Tomorrow named after. N.N. Priorova. Tel. 89037485782, e-mail: [email protected] Moscow, Priorova street, building 10, index 123480
Lazarev Anatoly Fedorovich – Doctor of Medical Sciences, Prof. head first department of the National Medical Research Center for Tomorrow named after. Priorova. e-mail: [email protected]
Ovcharenko Anton Vasilievich – head of the Center for Traumatology and Orthopedics, Emergency Hospital named after. Shevchenko, Kaluga. e-mail: [email protected]
Information about authors
Solod EI – MD, researcher of the First Department of National Medical Research Center of Traumatology and Orthopedics, Moscow.
Lazarev AF, – MD, professor of the Department of Trauma of National Medical Research Center of Traumatology and Orthopedics, Moscow.
Ovcharenko AV – Head of Center for Traumatology and Orthopedics, Kaluga.
Funding: The study had no sponsorship.
Funding: The study had no sponsorship.
Conflict of interest: The authors declare no conflict of interest.
Conflict of interests: The authors declare no conflict of interest.
For quotation:
Solod E.I., Lazarev A.F., Ovcharenko A.V., TREATMENT POSSIBILITIES FOR PATIENTS WITH PELVIC RING INJURIES // Department of Traumatology and Orthopedics. 2021.No3(33). With. 46-52.
General manifestations of a fracture
A fracture of the ischium is a serious, painful injury. The patient experiences traumatic shock with a sharp depression of the functions of all organ systems. Painful shock develops in more than a third of patients with a simple pelvic fracture. If the injury is combined with damage to the integrity of internal organs, a state of shock occurs in 100% of cases. It is manifested by pallor of the skin and mucous membranes, the appearance of cold sweat, a decrease in blood pressure along with an increase in heart rate, as well as fainting.
If you suspect damage to the ischium, place the victim in a frog position and place a bolster under his feet.
The following symptoms may appear immediately at the time of injury or after it:
- if the urethra is damaged by fragments of the ischium - bleeding from the genitals;
- impaired urine output;
- the appearance of an extensive painful hematoma;
- visual change in the structure of the pelvis - it becomes asymmetrical, but the patient cannot return it to its normal position;
- inability to support limbs;
- severe pain, which especially intensifies when trying to move the leg or transfer weight to it;
- if the intestinal walls are damaged, intestinal bleeding is observed;
- imbalance of normal intestinal microflora.
The first sign that a fracture has occurred with mixing is bleeding. In most cases, the patient remains in a state of shock after injury and may not feel pain. Pelvic fractures with and without displacement require urgent hospitalization, and you should not transport the victim yourself.
Discussion
Analysis of clinical data for 2 years suggests that before the advent of CT in the routine practice of examining patients, some pelvic fractures in elderly patients remained undetected and were treated with conservative methods. In all cases, when treating elderly patients, early activation is necessary to prevent hypostatic complications, combat pain and senile dementia. However, today, after establishing the correct diagnosis, the question remains open about the need to fix fractures using known methods of internal or external fixation. One of the main problems is the choice between the risks of surgical treatment and its benefits in the form of stabilization of the pelvic ring and the possibilities of early activation. Obviously, the main obstacle to early activation in elderly patients is pain. In addition, it is quite difficult to assess the intensity of pain in patients after various types of treatment due to the lack of objectivity of such a parameter as pain.
Russian authors report that minimally invasive fixation, activation and early rehabilitation can significantly reduce the number of complications and mortality [30]. According to A. Höch et al. [11], in 18% of cases in the surgical treatment group complications occurred, however, despite this, the 2-year survival rate was 82%, while in the conservative treatment group there were encouraging results (8% complications) and a disappointing survival rate of only 61%. . According to N. Kanakaris et al. [8], in most cases, preference is given to a conservative method of treatment, since the majority of fractures are considered mechanically stable and there are a limited number of fixation techniques in conditions of porous bone and aggravated somatic status of patients. In addition, the situation is aggravated by the insufficient number of qualified surgeons. A. Hoch et al. [13] revealed that the choice of treatment method is based on the patient’s age, regardless of the type of fracture: thus, surgical treatment is mainly carried out in the group of patients under 80 years of age, while older patients are treated with conservative therapy. For type C fractures, surgical interventions were performed in 50% of cases, which exceeds the rates of previous studies [31].
M. Rollmann et al. [17] believe that type B fractures with stable hemodynamics, the possibility of early activation and adequate pain relief must be treated conservatively, and type C fractures have the highest mortality rate and require surgical intervention.
This work shows the need for further study of the problem by conducting ethically and organizationally possible randomized scientific studies using conservative and surgical methods and subsequent comparison of results.
First aid to the victim
The first thing you can do to help the victim is to call an ambulance. While waiting, you should not try to analyze the injury, conduct tests or any other manipulations. Before the doctors arrive, it is recommended to be in the frog position - lie on your back, bend your legs at the knee joints and spread them apart. This way the pain will be less pronounced. To relieve pain and prevent swelling, you can take a pain reliever and apply a cold compress to the injured area.
Diagnostic methods
The purpose of diagnosis for pelvic fractures is to determine which bones were damaged and in what area. In addition, it is important to determine the nature of the fracture and the presence of complications. The first diagnostic test is radiography. The photographs clearly show all the bones and their fragments, as well as some internal organs.
For additional diagnostics of the urinary system organs, contrast agents are used. They are inserted into the lumen of the urethra, and then pictures are taken. In this way, the integrity of the urinary tract can be determined. If damage to the bladder is suspected, it is examined using cystography.
Treatment
Treatment of a fracture of the ischium is a set of measures aimed at restoring its integrity. First of all, the patient must be taken to the hospital and at the same time try not to provoke mixing of bone fragments. In a hospital setting, the patient is in a supine position, in a frog position, and his legs are placed on a low bolster.
Conservative treatment
Non-surgical treatment is possible for uncomplicated fractures if there is no risk of complications. The first condition for the treatment of all fractures is immobilization of the damaged bone. For tubular bones of the limbs it is convenient to use plaster casts, but for pelvic injuries this option is not available. There are several options for fixing the ischium:
- a fixing hammock that supports the lower back and pelvis, removing all stress from it;
- Beler splints - a rigid structure that prevents all movement of the patient in the area of the fracture.
To restore bone integrity, the victim must spend at least several months in fixation structures
Provided that the bones are securely fixed, healing occurs within 2-3 months. Treatment can be continued at home, but it is important to follow all doctor’s recommendations.
Surgical intervention
Surgery is necessary to treat complicated fractures with damage to internal organs. During the intervention, the surgeon stops the bleeding, sutures the wounds and treats them with disinfectant solutions. In addition, the integrity of the bones can be restored surgically - for this you will need metal plates.
Medicines
Drug therapy is prescribed for both conservative and surgical treatment of pelvic fractures. The patient may be prescribed the following groups of drugs:
- antibiotics - to destroy pathogenic microflora and prevent it from entering the wound;
- anti-inflammatory and painkillers;
- calcium and phosphorus preparations, vitamins;
- chondroprotectors - tablets or ointments that stimulate the regeneration of cartilage and bone tissue.
The course of taking medications can continue long after the fixatives are removed. At this stage, products can be used in the form of ointments or creams.
Medicines
When undergoing conservative treatment or after a previous operation, a person must be prescribed medications.
In this case he is prescribed:
- antibiotics. They help destroy bacterial cells, prevent bacteria from entering the site of damage;
- anti-inflammatory, painkillers;
- medications with calcium, phosphorus, vitamin complexes;
- chondroprotectors. They are prescribed in tablets, creams, ointments. They improve the process of regeneration of cartilage and bone tissue.
Remember: experts recommend taking medications until the fixing devices are removed.
Rehabilitation after fractures
An equally important stage is recovery after a fracture. The pelvic bones will not be able to immediately bear a large load, so you will have to return to your normal life gradually. Doctors have several recommendations on how to quickly rehabilitate and get in shape after a fracture of the ischium:
- physical therapy - exercises to develop the strength and elasticity of muscles and ligaments; they should not be accompanied by painful sensations;
- physiotherapy - procedures to improve blood circulation, lymphatic drainage and regenerative processes in cells, due to which they are quickly renewed;
- massage - useful only after eliminating acute inflammation and pain;
- diet - the diet should contain a large amount of foods with calcium and vitamin D (dairy and fermented milk products, cheese, nuts, vegetable oils, fish and others).
A fracture of the ischium is a serious injury. Even after recovery, you can forget about serious sports and intense physical activity. Bones remain fragile and prone to damage, especially in old age.
Possible complications
If treated promptly, non-displaced pelvic fractures are treatable. However, in difficult cases, in the presence of fragments and displacement of fragments, dangerous consequences of a fracture may occur:
- insufficient rate of fusion of fragments;
- bone fusion in the wrong position;
- impaired sensitivity of the lower extremities;
- shortening of legs;
- contracture (immobility) in the hip joints;
- entry of bacterial microflora and development of purulent inflammation;
- the need for additional therapeutic measures to restore damaged internal organs.
A fracture of the pelvis and ischium is a dangerous injury. Compared to injuries to other skeletal bones, it occurs much less frequently, but more often causes dangerous consequences. If you suspect a fracture of the pelvic bones, it is not even recommended to provide first aid to the victim - this can provoke displacement of bone fragments and injury to internal organs. The treatment is long, and even after full recovery the patient still has a list of limitations.
How long does it take for a pelvic fracture to heal?
A pelvic fracture is a serious injury, the outcome of treatment of which determines the future fate of a person. If the treatment is incorrect or the patient does not follow medical instructions, the bones may heal incorrectly and cause permanent problems in the future.
In general, it can take four to six months for the pelvic bones to heal and recover from injury, but for severe injuries, full recovery can take years. Despite advances in the field of modern traumatology, the number of people with disabilities after pelvic injuries remains quite significant (approximately 15%). In addition, pelvic injuries almost always derail the careers of professional athletes.
Although there is no specific time frame for complete healing of such injuries, there are a number of factors that are taken into account when making a prognosis.
These include the following:
- Type of fracture: open or closed.
- The location of the damage and the number of injured bones and tissues.
- Level of blood supply to damaged bones.
- Age of the victim: It can take six months for the bones of adults to heal, but only one for children.
- General health: level of bone mineralization, blood and muscle tissue.
- Presence of aggravating factors: bad habits, concomitant and chronic diseases, etc.